Comprehensive Handbook of Psychological Assessment, Volume 2: Personality Assessment Mark J. Hilsenroth (Editor), Daniel L. Segal (Editor), Michel Hersen (Editor-in-Chief) ISBN: 978-0-471-41612-8
September 2003
Part Five: Specific Content Areas
33 Projective Assessment of Object Relations 449 George Stricker and Jane Gooen-Piels
34 Projective Assessment of Defense Mechanisms 466 John H. Porcerelli and Stephen Hibbard
35 Projective Assessment of Interpersonal Dependency 476 Robert F. Bornstein
36 Projective Assessment of Borderline Psychopathology 485 Mark A. Blais and Kimberly Bistis
37 Projective Assessment of Psychological Trauma 500 Judith Armstrong and Nancy Kaser-Boyd
38 Projective Assessment of Suicidal Ideation 513 Daniel J. Holdwick Jr. and Leah Brzuskiewicz
39 Projective Assessment of Disordered Thinking 526 James H. Kleiger
Projective Assessment of Object Relations
GEORGE STRICKER AND JANE GOOEN-PIELS
RORSCHACH MEASURES 450 Developmental Analysis of the Concept of the Object Scale (DACOS) 450 Mutuality of Autonomy Scale (MOAS) 451 TAT-BASED MEASURES 452 Social Cognition and Object Relations Scale (SCORS) 452 DREAM-BASED MEASURES 454 Object Representation Scale for Dreams (ORSD) 454 MEAURES BASED ON EARLY MEMORIES 455 Early Memories Test (EMT) 455 Comprehensive Early Memories Scoring System (CEMSS) 456 PARENTAL REPRESENTATIONS 456 OTHER, LESS USED APPROACHES 457 Rorschach-Empathy-Object Relationship Scale (RE-ORS) 458
Stricker and Healey (1990) presented a comprehensive review of the empirical literature on the projective assessment of object relations including Rorschach, TAT, and dreambased measures, as well as measures based on early memories, among others. This chapter incorporates Stricker and Healey’s findings, reporting on the continued evolution to date of the measurements they reviewed and presenting any additional empirical literature on instruments that have emerged in the literature.
Understanding the broad realm of object-relations theory helps to conceptualize the way in which these measures can contribute to an understanding of an individual’s objectrelational domain. Object-relations theory is not a singular construct, and draws upon ego psychology, self-psychology,
Personal Sphere Model (PSM) 458 Measurement of Symbiosis 458 Comprehensive Object Relations Profile (CORP) 458 Psychoanalytic Rorschach Profile (PRP) 459 Separation-Individuation Theme Scale (SITS) 459 Boundary Disturbance Scale (BDS) and Thought Disorder Scale 459 Differentiation-Relatedness Scale 460 Transitional Object Early Memories Probe 460 The Dietrich Object Relations and Object Representations Scale (DORORS) 460 CONCLUSION 460 REFERENCES 461
and developmental and cognitive theories. It is multidimensional and therefore operationalized in many ways. For example, object relations incorporates object representations, level of separation and individuation, and the degree to which the other person is experienced as a whole person or a partobject present to gratify needs. Each component of object relations gives one angle of perspective into an individual’s object relations. An individual’s quality of object relations is understood as shaping how he or she understands interactions with others, which in turn influences how these interactions are consequently carried out. Object relations are understood to manifest in the cognitive, affective, and interpersonal domains (Lerner, 1998). Each object-relations measure, therefore, is a nomothetic tool that helps to assess parts of these domains and, in so doing, shapes an ideographic understanding of an individual (Stricker & Gold, 1999). The choice of nomothetic tool to select is based on the referral question and type of experience one wishes to access in the individual (Stricker & Gold, 1999). Furthermore, the validity of such an instrument is not determined without context, but within the context of the purpose for which the test is being applied (Stricker & Gold, 1999).
Measurement devices described in this chapter are projective, and so by definition are applied to data that emerge from an individual’s unconscious domain. Only projective measurement used with adults will be presented. Many of these measures are also used with children and adolescents (i.e., Mutuality of Autonomy Scale, Krohn’s Object Representation Scale). However, although their contributions are meaningful, reliability and validity data resulting from studies with these populations are not presented.
RORSCHACH MEASURES
In the original review (Stricker & Healey, 1990) and in this update, the majority of projective object-relations measures were based on scores that were developed for Rorschach responses.
Developmental Analysis of the Concept of the Object Scale (DACOS)
Blatt, Brenneis, Schimek, and Glick (1976) developed a procedure for evaluating the developmental level of human responses on the Rorschach. This measure has been referred to as the Developmental Analysis of the Concept of the Object Scale (DACOS) and as the Concept of the Object on the Rorschach Scale (CORS). This system can be applied to a variety of data forms, including dreams, open-ended descriptions, TAT stories, and, most often, Rorschach responses (Stricker & Healey, 1990). Blatt’s scale is based on the theoretical conceptualization of developmental psychoanalysis and cognitive developmental psychology and is aimed at studying object and self-representations. This system’s aim is to assess the structure of representations by means of a content approach to analyzing Rorschach data. Specifically, it scores human responses along three primary dimensions, including differentiation, articulation, and integration (Blatt & Ford, 1994). Within each dimension, developmental levels are reflected along a continuum. Differentiation corresponds to whether the figure seen is a full human, a full quasi-human, or a part of a human or quasi-human figure. Articulation refers to attributions that are ascribed to the figures and the degree to which those attributions are described in terms of manifest physical or functional attributes. Integration is based on the degree to which action is internal, is integrated with the object, and is an integrated interaction with another object (Blatt & Ford, 1994). (For more detailed description of the scale, see Blatt et al., 1976; Blatt & Ford, 1994; Blatt & Lerner, 1983b.)
Reliability
A range of interrater reliabilities have been reported, including 75% for perceptual articulation, 96% for differentation, and 97% for an unspecified dimension (Stricker & Healey, 1990). Scores across all domains generally have fallen in the range of the upper 80s to mid-90s. Some studies, however, do not give complete reliability data and report only range and average reliability score. Stricker and Healey (1990) note that the reliability scores for this scale are acceptable, and the various subscales’ reliability seems to be replicated consistently. Blatt and Ford (1994) report reliability estimates in both clinical and normal samples to range from .86 to .97 (item alpha ! .70). Hibbard, Hilsenroth, Hibbard, and Nash (1995) report interrater reliability ranging from .84 to .95.
Validity
Stricker and Healey (1990) report on Blatt’s original study (Blatt et al., 1976), in which Rorschach records were obtained in a sample of 37 normal patients at four intervals across 20 years. Results revealed significant developmental changes in conjunction with changes in human responses on the Rorschach. Investigators found an increase over time in “the number of accurately perceived, well articulated, full human figures involved in appropriate, integrated, positive and meaningful interactions” (Blatt et al., 1976, p. 371, as cited by Stricker & Healey, 1990, p. 220).
Stricker and Healey (1990) found that most of the research with the DACOS focused on differentiating diagnostic categories. They reported on the ability of the scale to differentiate between normals and patients (Blatt et al., 1976); psychotic and nonpsychotic patients (Ritzler, Zambianco, Harder, & Kaskey, 1980); schizophrenics and borderlines (Spear, 1980; Spear & Sugarman, 1984); neurotics, outpatient borderlines, inpatient borderlines, and schizophrenics (Lerner & St. Peter, 1984a, 1984b); restricting and bulimic anorexics (Piran, 1988; Piran & Lerner, 1988); and narcissists and borderlines (Farris, 1988). The scales also were used to describe opiate addicts’ interpersonal characteristics as compared to neurotic and psychotic clinical samples (Blatt, Berman et al., 1984; Blatt, McDonald, Sugarman, & Wilber, 1984), as well as the change
resulting from treatment (Blatt, Ford, Berman, Cook, & Meyer, 1988; Schwager & Spear, 1981). Research conducted since Stricker and Healey’s (1990) review includes a study by Stuart et al. (1990) that used the DACOS to successfully distinguish between borderline and mood-disordered patients and a normal comparison group.
Cook, Blatt, and Ford (1995; Blatt & Ford, 1994) reported on a study predicting therapeutic response with 90 seriously disturbed young adults. Results indicated that psychological processes captured through the DACOS assessment of representational dimensions predicted response to treatment.
Hibbard et al. (1995) used the DACOS to evaluate the construct validity of the concept of object relations. They correlated the DACOS with Westen’s Social Cognition and Object Relations Scale (1991a, 1991b; reviewed later in this chapter), factoring out any variance resulting from psychopathology or intelligence level. Results supported the construct validity of object representations and the validity of the DACOS as a measure of that construct.
The DACOS also has been used in the assessment of other projective data, including dreams. In a recent study by Kern and Roll (2001), the DACOS was used with dream data to evaluate the relationship between culture and internalized object representations. Although the hypothesized differences between cultures were not confirmed, differences between sexes emerged across all developmental dimensions.
Mutuality of Autonomy Scale (MOAS)
Urist (1977, 1980) developed the Mutuality of Autonomy Scale (MOAS) to assess levels of object relations in a developmental model via the analysis of Rorschach data. This method has its theoretical underpinnings in the writing of Kohut (1966, 1971, 1977) and Kernberg (1966, 1975, 1977), more specifically in their understanding of borderline and narcissistic conditions, reflecting self-psychology, ego psychology, and object-relations theory. This seven-level scale, scoring responses involving interaction of human, animal, or inanimate percepts, sorts Rorschach responses into categories that reflect the quality of relationships in the Rorschach responses. The scale focuses on the developmental movement toward separation-individuation (see Urist, 1977, for definition of scale points.)
Urist and Schill (1982) summarized the scale somewhat differently at a later point, but the overall intent remained the same as with their original definitions. Altered scale points included Reciprocity-Mutuality; Collaboration-Cooperation; Simple Interaction; Anaclitic-Dependent; Reflection-Mirroring; Magical Control-Coercion; and Envelopment-Incorporation (Stricker & Healey, 1990).
Reliability
Urist reported interrater reliability scores of .52 for exact agreement, .66 for agreement within one-half point, and .86 for agreement within 1 point (Stricker & Healey, 1990). Other researchers report reliability statistics of exact agreement ranging from .58 to .90 and 1-point agreement from .72 to .98 (Stricker & Healey, 1990). Fowler, Hilsenroth, and Handler (1996a) report interrater reliability for the MOAS to be .90 In a review of the MOAS, Holaday and Sparks (2001) report on a range of interrater reliability from 52% reported by Urist to 91% reported by Berg, Packer, and Nunno (1993). An average rate of agreement of MOAS reliability of 74.3% was found across all studies reported by Holaday and Sparks (2001). These researchers suggested that existing guidelines found in the literature presented scoring difficulties and proposed revised guidelines that would not alter the validity of the scale or change the levels for scoring the MOAS. In a test of their revisions, they found an improvement in interrater agreement scores from 67% using original guidelines to 80% agreement. However, these researchers note the need for further research to examine whether MOAS levels should be collapsed or other scoring categories added.
Validity
Urist’s (1977) evidence for construct validity includes significant correlations between the MOAS and autobiographical data and staff ratings of inpatients when similar scoring guidelines were used (Stricker & Healey, 1990).
Stricker and Healey (1990) present research on the MOAS that explored similarities between transsexuals and borderlines (Murray, 1985); the use of the MOAS, with a modified 10-point scale, to successfully differentiate between subgroups of borderline pathology (Spear & Sugarman, 1984); the utility of the scale to differentiate both restricting and bulimic anorexics from controls (Strauss & Ryan, 1987); and the ability of the scale to use childhood MOAS scores to predict rehospitalization as adults later in life (Tuber, 1983). These authors note the findings of Kavanagh (1985) that indicate the MOAS did not differentiate between treatment with psychoanalysis and treatment with psychoanalytic psychotherapy. Blatt et al. (1988) found that, when the MOAS was used to measure change resulting from treatment, it did not reflect a significant difference, only a tendency for fewer malevolent responses in borderlines and schizophrenic young adults (Stricker & Healey, 1990).
Stricker and Healey (1990) present findings that the MOAS reflected pathology observed in inpatients at the time of their hospitalization and across their lifetime, but not at the time the assessment was conducted (Harder, Greenwald, Wechsler, & Ritzler, 1984). They note the suggestions of the study’s authors that the MOAS may be used to indicate potential for pathology. Blatt, Tuber, and Auerbach (1990) supported this finding. They found that the MOAS had a significant correlation with independent assessment of clinical symptoms but not of interpersonal behavior (Stricker & Healey, 1990), and concluded that the MOAS may be more appropriate as an indicator of pathological functioning and not an assessment of object relations.
Blatt et al. (1990) present data to support convergent validity (Stricker & Healey, 1990). They found significant correlations between the mean MOAS score and the developmental level of inaccurately perceived responses (OR!) scale of the DACOS. The mean developmental score for OR! predicted the mean MOAS score. The mean MOAS score was not significantly correlated with either the weighted sum or the mean developmental level of accurately perceived responses (OR#). Blatt et al. state that the mean score of the MOAS is the most differentiated of the scores of the MOAS. Stricker and Healey (1990) note the appearance that the MOAS measures some, but not all, of the same elements as the DACOS.
Using the MOAS, Berg et al. (1993) found significant correlations between composite scores of severe thought process disturbance and severe imbalance in internalized object representations.
The MOAS has been used to differentiate diagnostic groups. Fowler et al. (1996a) used the MOAS to assess construct validity and clinical utility of the Early Memory Dependency Probe. The MOAS-High score significantly differentiated the three groups under examination. Blais, Hilsenroth, Fowler, and Conboy (1999) examined patients with antisocial, borderline, histrionic, and narcissistic personality disorders to explore the relationships of select conceptually derived Rorschach scales, including the quality of object relations, to the DSM-IV bipolar personality disorder criteria. Results indicate that the MOA variable (MOA-H) was among three variables (Rorschach Oral Dependency and Devaluing) that were exclusively associated with the bipolar personality disorder total score, supporting its use to differentiate among the four personality disorders examined. Blais, Hilsenroth, Castlebury, Fowler, and Baity (2001) examined the incremental validity of Rorschach variables, including the MOAS, and the Minnesota Multiphasic Personality Inventory-2 (MMPI-2) to predict DSM-IV antisocial, borderline, histrionic, and narcissistic personality disorder criteria. With the other two variables, Rorschach Oral Dependency and Devaluing, the MOAS accounted for an additional 30% of the variance beyond the MMPI-2 BPD-O scale in the bipolar personality disorder criteria score. These results provide support for the criterionrelated validity of the MOA-H.
Fowler, Hilsenroth, and Nolan (2000) used the MOAS to assess the object representations of self-mutilating borderline patients compared with non-self-mutilating borderline patients, as a means to understand this malevolent behavior and its continuation. Self-mutilating borderline patients were found to manifest more instances of malevolent, controlling object representations.
TAT-BASED MEASURES
Only a single measure, based on the work of Westen (1985/ 1989), has been based on TAT responses. However, it is of great importance because it has generated good supportive data and it also has been applied to data from measures other than the TAT.
Social Cognition and Object Relations Scale (SCORS)
The Object Relations and Social Cognition Scale remains the most comprehensive scoring system developed primarily for object-relations assessment in the TAT since Stricker and Healey’s (1990) review. Since Stricker and Healey’s review (1990), the scale has appeared in the literature under the name the Social Cognition and Object Relations Scale (SCORS; Conklin & Westen, 2001). The theoretical underpinnings of this scale are psychoanalytic object-relations theory and social cognition research (Westen, 1991b; Westen, Lohr, Silk, Gold, & Kerber, 1990). Westen and colleagues (Conklin & Westen, 2001) have recently developed a revised version of the SCORS (SCORS-R), but reliability and validity information is currently not available. Therefore, we will comment only briefly on the SCORS-R and will maintain the focus of our discussion on the SCORS.
The SCORS taps four dimensions of object relations: Complexity of Representations of People, reflecting the quality of differentiation of representations; Affect-Tone of Relationship Paradigms, reflecting the quality of interpersonal interactions along the continuum from malevolent to benevolent; Emotional Investment in Relationships and Moral Standards, reflecting the degree to which others are experienced as need gratifiers versus whole individuals separate from the respondent, as well as the level of development of moral standards and how those standards influence behavior; and Understanding of Social Causality, reflecting the degree to which attributions about social interactions, understanding the causes for the occurrence, and accompanying self-thoughts and feelings are accurate, logical, and psychologically minded (Westen, 1991a). Each dimension is rated using a 5-point scale, with higher numbers indicating greater level of maturity of object-relations development and healthy functioning. A manual has been developed detailing the scoring procedures (Westen, 1985/1989, as cited by Stricker & Healey, 1990). Except for the Affect-Tone of Relationship Paradigms dimension, each dimension is theorized to follow a developmental progression (Conklin & Westen, 2001).
As described by Conklin and Westen (2001), the SCORS-R is similar to the SCORS, but taps six dimensions instead of five. Three of the dimensions are the same as in the SCORS, Complexity, Affect-Tone, and Social Causality. The Investment in Relationships and Moral Standards dimension is broken down into two dimensions in the SCORS-R. One dimension addresses relationships and the other values and moral standards. An additional dimension has been added, Dominant Interpersonal Concerns, that assesses interpersonal fears, wishes, and concerns. Revisions were made to the SCORS to make the instrument easier to use and to add a thematic component of content assessment (Conklin & Westen, 2001).
Reliability
Conklin and Westen (2001) report that research consistently finds interrater reliability of the SCORS to be above .80 as assessed by both Pearson’s r and the intraclass correlation coefficient. They also report strong internal consistency, as assessed by Cronbach’s alpha, in particular for the more cognitive dimensions.
Validity
A number of validation studies have been reported on the SCORS, demonstrating both good concurrent and construct validity. Stricker and Healey (1990) report on Westen’s (1985/ 1989) description of validation research with both normal and clinical populations as follows. In one study, clinical psychology students were found to score higher than natural science graduate students on Complexity and Social Causality. Both scales also correlated with measures of psychological mindedness. In a second study, borderline personality disorder was differentiated from major depression, with the Affect-Tone dimension found to be the most discriminating scale. Analysis of discriminant function resulted in 80% accuracy, based on six TAT cards. The Complexity and Social Causality scales correlated with Blatt’s Complexity subscale, and the Affect-Tone dimension correlated with Blatt’s Malevolence and Ambivalence subscales. As reported by Stricker and Healey (1990), these scales have been found to predict social adjustment, clinician-rated interpersonal pathology, and the relevant symptom scales on the revised Symptom Checklist-90 (Derogatis, 1977). Westen (1991a) reports on the measure’s ability to successfully distinguish borderline patients from psychiatric and normal comparison patients, with discriminant function analyses yielding 80% accuracy for discriminating borderlines from each of the comparison groups, using responses to five of seven TAT cards.
Porcerelli, Hill, and Dauphin (1995) used the Capacity for Emotional Investment (CEI) dimension to successfully differentiate participants classified as normal, sociopathic, and psychotic. Ackerman, Clemence, Weatherill, and Hilsenroth (1999) found that the SCORS variables were able to differentiate patients with antisocial, borderline, narcissistic, and Cluster C personality disorders. In another study, Ackerman, Hilsenroth, Clemence, Weatherill, and Fowler (2000) used the SCORS to predict number of psychotherapy sessions attended.
Convergent validity has been demonstrated in a number of studies. The four scales of the SCORS have been found to correlate with similar scales applied to interview data, including early memories, psychiatric interviews, or psychotherapy transcripts (Westen, 1991a). Variables of the SCORS correlate in predicted ways with validated research instruments, including the Loevinger Sentence Completion Test and Weissman’s Social Adjustment Scale (Conklin & Westen, 2001). Predicted associations have been found between SCORS variables, the Affect-Tone of Relationship Paradigm in particular, and childhood experiences of disrupted attachments, the number of times a family moved during the patient’s childhood, and sexual abuse (Conklin & Westen, 2001).
Hibbard et al. (1995) report on a validity study focusing on the construct validity of object representations as well as the convergent validity, in which the SCORS and Concept of the Object on the Rorschach (COR) were compared with
each other as well as with measures of intelligence and psychopathology. Results support the construct validity of the SCORS, as the Complexity and Social Causality subscales correlated reliably only with the subscales of the COR that are sensitive to differentiation, complexity, and elaboration of human figures and their actions on the Rorschach. Findings also support the construct validity of object representations and the validity of the SCORS as a measurement of that construct, as well as the SCORS as a valid measurement of the construct of the cognitive-structural aspect of human object representation itself. Although results did not support a structural-cognitive link to psychopathology, the SCORS Affect-Tone and Capacity for Emotional Investment dimensions detected differences between more and less severely personality-disordered groups.
In a study assessing complexity of representations Leigh, Westen, Barends, Mendel, and Byers (1992) found that the measure of Complexity of Representations applied to the TAT converged with description of actual experience, supporting construct and convergent validity. Convergent validity has been assessed through correlations between TAT and interview ratings for Affect-Tone (Barends, Westen, Leigh, Silbert, & Byers, 1990) and through correlations between the SCORS dimensions and related scales (Westen, Huebner, Lifton, & Silverman, 1991).
Correlations with Blatt, Wein, Chevron, and Quinlan’s (1979) measure of complexity provided evidence for convergent validity as well. There was a lack of overall correlations with the more affective measures of Blatt et al.’s measure, which lends further support to discriminant validity. Ackerman, Hilsenroth, Clemence, Weatherill, and Fowler (2001) explored the convergent validity of object-relations scales, including the SCORS. Results support convergent validity between the Rorschach and TAT, specifically supporting the use of these measures to assess object relations.
DREAM-BASED MEASURES
One measure was based on dreams (Krohn & Mayman, 1974) and is not used very frequently. However, the conceptual approach has also been used with the Rorschach and with early memories, so it has more importance than is immediately obvious.
Object Representation Scale for Dreams (ORSD)
As noted by Stricker and Healey (1990), Mayman and his colleagues (e.g., Mayman, 1967) focused on thematic aspects of affective experience to assess object relations with the Rorschach. Their measurement is also applied to early memories (Mayman & Faris, 1960) and dreams. Ego psychological theory, in particular the contributions of Mahler (Mahler, Pine, & Bergman, 1975) and Kernberg (1975), form the bases on which Mayman’s work is developed (Stricker & Healey, 1990). Blatt and Lerner (1983a) present Mayman’s approach as being based on the clinical intuitive method, which he applied to new sources of data in the study of object relations (Stricker & Healey, 1990). In this chapter, we will focus mostly on Mayman’s work in relation to dreams and early memories.
Mayman’s Object Representation Scale for Dreams (ORSD) is a hierarchical measure that assesses an individual’s perception of others across an 8-point ordinal scale that assesses others as fragmentary, absent, and alienated, at one end, to complete, differentiated, and alive, at the other (Stricker and Healey, 1990). The continuum of this scale moves along various stages of object relations from primary narcissism to empathic object relatedness (Levine, Tuber, Slade, & Ward, 1991). This scale has also been referred to in the literature as the Krohn Object Representation Scale for Dreams (Krohn & Mayman, 1974). The scale was developed to evaluate the overall level of maturity of an individual’s object representation and it is applied to depictions of human figures in written reports of dreams (Levine et al., 1991). When not applied to dreams, it is simply called the Krohn Object Representation Scale (Levine & Tuber, 1993).
The ORSD moves on a continuum with one end reflecting the individual’s internal object world experienced as lifeless, alien, unpredictable, desolate, and essentially without people, and the other reflecting human beings experienced in fully human, differentiated, and complex ways (Levine and Tuber, 1993). (Extended descriptions of scale points are available in Krohn and Mayman [1974] and Hatcher and Krohn [1980].)
Reliability
Interrater reliability is reported by Krohn and Mayman (1974) to range from .58 to .79 for exact agreement and from .74 to .89 for agreement within 1 scale point, using the Rorschach test, dreams, and early memories (Stricker & Healey, 1990). Ryan (1974) developed a similar scale comprised of 20 scale points and applied to early memories, reporting .80 and .86 reliability (Ryan & Bell, 1984; Ryan & Cicchetti, 1985, as cited by Stricker & Healey, 1990). Spear (1980) reported 83% for percentage of exact agreement when the measure was applied to Rorschach data and 80% when applied to dreams (Stricker & Healey, 1990).
Validity
Stricker and Healey report the following studies of the ORSD validity. ORSD criteria applied to Rorschach data discriminated hysterical/impulsive borderline patients from obsessive/ paranoid borderline patients, but when applied to dreams and Blatt’s DACOS, it only discriminated schizophrenics from borderline patients, with no discriminatory success between borderline subgroups. As a test of convergent validity, data from Rorschach, early memories, and dreams were examined in relation to one another, as was the relationship between these measurements and therapist-supervisor ratings of the patient’s level of object relations. Results show high intercorrelations, thus indicating the meaningful relationships between these variables (Krohn & Mayman, 1974). Partial correlations indicated that the primary sources of object-relations data were dreams and early memories, as contributions by the Rorschach data to the correlations were minimal. However, the Rorschach did predict a combined level of object relations and psychopathology. Frieswyk and Colson (1980) also contributed to the research on construct validity. Their results indicated that, when the ORSD was applied to Rorschach data, global improvement in hospitalized patients was predicted and, in specific, the data predicted termination levels of object relations, the state of the therapeutic alliance, and ratings of healthsickness.
Ryan and Bell (1984) demonstrated discriminant validity using their adapted version of the ORSD. Although they found nonsignificant correlations between the object-relations measure and psychiatric severity, when following patients from psychotic phase through to their recovery, their measure was able to discriminate changes in levels of object relations. In a study aimed at understanding the therapeutic alliance, Ryan and Cicchetti (1985) found that the quality of object relations accounted for approximately 30%, the greatest part of the variance, of the quality of therapeutic alliance.
MEASURES BASED ON EARLY MEMORIES
In many ways, early memories are similar to dreams and even to TAT stories, and so many of the approaches in these three categories show striking similarities.
Early Memories Test (EMT)
The Early Memories Test (Mayman, 1968; Mayman & Faris, 1960) uses earliest memories as a tool to tap into unconscious material that denotes object representations of self and other. Experimental learning theory of Sir Frederick Bartlett (Bartlett, 1932, as cited by Fowler, Hilsenroth, and Handler, 2000) was the original concept on which Mayman based the reconstructive nature of early memories, but he later turned to psychoanalytic theory, wherein the projective quality of memories could be understood (Fowler et al., 2000). In regard to the revealing nature of early memories, Nigg et al. (1992) noted, from Mayman (1968) and Mayman and Faris (1960), “when subjects narrate on the EMT a handful of early memories from a wealth of early experiences, they do so in a manner consistent both with their personality organization and with their view of their interpersonal or object world” (p. 61). Although Mayman’s (1968) systematic approach to obtaining early memories involved 16 queries, including recall of unstructured memories and circumscribed events, later investigators adapted the traditional queries as required by the area of personality they were seeking to explore (Fowler et al., 1995).
Nigg et al. (1991, 1992) used data from the EMT to evaluate object representation in borderline patients with and without depression compared to nonborderline patients with either major depression or no psychiatric diagnosis. As one
of their study goals, object representations of sexually abused patients with borderline personality disorder (BPD) were assessed to examine the relationship between BPD and reported histories of sexual and physical abuse. Results indicated that a reported history of sexual abuse predicted extremely malevolent representations and representations involving deliberate injury in reported earliest memories. The representations that emerged were also discriminative between borderline patients who had reported sexual abuse histories compared to those who did not. The second study goal involved the assessment of malevolent object representations as a means to discriminate between these patient and nonpatient groups. Borderline patients were discriminated from nonborderline patients based on the presence of more malevolent representations.
Fowler et al. (1995) conducted two empirical studies to test the validity of novel queries they incorporated into the EMT aimed at assessing object relations. They used the Complexity of Representation and Affect-Tone dimensions of the SCORS to assess psychological development of a person’s representational world. Their second study assessed the construct validity of the EMT by comparing the Affect-Tone and Complexity of Representation scores with projective and objective measures that assessed similar constructs (including MOAS and the Holt Primary and Secondary Process Aggression Scale). Results of the first study indicated that the novel queries could distinguish between the clinical and nonclinical group. Results of the second study supported the construct validity of the early memories.
Comprehensive Early Memories Scoring System (CEMSS)
The development of the Comprehensive Early Memories Scoring System (CEMSS) is based on Mayman’s orientation toward ego psychology. Developed by Last (1983, as cited by Stricker & Healey, 1990) and reported by Last and Bruhn (1983, 1985), it was first applied to a child population, which is beyond the scope of this chapter. We will incorporate reliability and validity findings from their initial development of the scale, however, because those results form the basis for its application with an adult population. This scale is comprised of nine categories, one of which assesses object relations and encompasses 48 items. Subcategories contained within the object-relations dimension include Perception of Others, Perception of Self, Perception of Environment, Individual Distinctiveness, and Degree of Interpersonal Contact. The range of ratings for each subcategory is 1 to 3. Three reflects the most differentiated response. Scores of all the subcategories are summed resulting in a unitary object-relations score.
Reliability
Stricker and Healey (1990) reported findings of interrater reliability for 188 early memories across all 48 items to be 92.6%. Across categories, agreement ranged from 64.2% to 100%. However, there was no report of the specific reliabilities for the object-relations subcategory.
Validity
Last and Bruhn (1983, 1985) demonstrated that the scale was successful in distinguishing various diagnostic groups from each other. Furthermore, type of pathology could be distinguished by content variables, and degree of pathology could be assessed by structural variables.
PARENTAL REPRESENTATIONS
Stricker and Healey (1990) reported on a method for assessing structural and qualitative dimensions of object representations, as developed by Blatt et al. (1979), that is based on an integration of the cognitive developmental work of Piaget (1956) and Werner (1948) and on object-relations theory. At the time that Stricker and Healey (1990) reviewed this method, assessment was based on the evaluation of seven traits, on a 7-point scale, that assessed spontaneous descriptions of parental figures. Also evaluated was the degree of ambivalence noted, which was scored on a 9-point conceptual level ranging from Point 1, others are seen as primarily need gratifiers or frustrators, to Point 9, others are described in terms that reflected a complex, whole, integrated human being. Since Stricker and Healey’s review, the assessment of parental representations by Blatt and colleagues has been presented in various ways. For example, Blatt, Wiseman, Prince-Gibson, and Gatt (1991) present a study in which the presence of 12 qualities, “Scorable Attributes,” describing the figure are assessed on a 7-point scale, and a “Conceptual Level” evaluating developmental cognitive level of the representation is assessed on a 9-point scale, ranging from a sensorimotorpreoperational to a conceptual level (Blatt et al., 1991). Quinlan, Blatt, Chevron, and Wein (1992) presented a refinement of the scale, including a revised rating procedure, in which three factors emerge, including Benevolent, Punitive, and Ambitious. In a later study conducted by Blatt, Stayner, Auerbach, and Behrends (1996), the Conceptual Level and Scorable Attributes are broken out into stand-alone scales: the “Conceptual-Level Scale” and the “Qualitative-Thematic Scale.” Degree of ambivalence is also assessed, as are the three underlying factors that emerged in their earlier study.
Reliability
Stricker and Healey (1990) reported reliability scores from Blatt et al. (1979) ranging from .68 to .93. Reliability for the conceptual level is reported as .85. They note similar reliabilities reported by Bornstein, Galley, and Leone (1986). Blatt et al. (1991) reported reliabilities ranging from .45 to .93, with an average reliability of .75, for the Scorable Attributes and .88 for the Conceptual Level. Quinlan et al. (1992) reported reliabilities ranging from .45 to .92, with a median reliability of .81. Reliability for ambivalence was assessed only at .41. On the three factors that emerged, the Benevolent, Punitive, and Ambitious scales, good interrater reliability was reported, but the intratest homogeneity coefficient, although quite high for the Benevolent scale, was only moderate for the Punitive and Ambitious scales. For further information on the comparison of the revised scale to the earlier version, see Quinlan et al. (1992). Blatt et al. (1996) reported .80 interrater reliability of the Conceptual Level, and the range of interrater reliability of the 12 qualities comprising the Qualitative-Thematic scales to range from .82 to .95. Interrater reliability for the degree of ambivalence expressed was .82. Levy, Blatt, and Shaver (1998) found interrater reliability to be .75 or greater for ratings of each of the 12 traits of the Qualitative-Thematic scales, the three derived factors, Ambivalence, Conceptual Level, and Scorable Attributes.
Validity
Stricker and Healey (1990) reported on the following studies. Relationships are reported by Blatt et al. (1979) between depression and lowered conceptual scores for parental descriptions, and between depression and parents described as lacking in nurturance, support, and affection. High “oral” patients were found by Bornstein et al. (1986) to give more negative descriptions of their mothers, but there were no differences found between high and low orals on Conceptual Level. Quinlan et al. (1992) found that the parental descriptions scales’ correlations with the Semantic Differential provide evidence for the convergent and discriminant validity of the technique. Blatt et al. (1991) found changes in clinical functioning of severely disturbed adolescents and young adults were in concert with significant change in the Conceptual Level and the degree of differentiation and articulation with which they described their parents. Blatt et al. (1996) found important structural changes in representations in descriptions of caregiving others that were in keeping with improvement in therapeutic progress. Hernandez, Hinrichsen, and Lapidus (1998) found an association between object relations and more adaptive coping and level of distress in adult caregiving children, and found poorer object relations in adult children whose mothers had a history of depression. Levy et al. (1998) found parental representations of securely attached participants were more positive in content and more conceptually complex, characterized by benevolence, nonpunitiveness, differentiation, and elaboration, compared to the insecure attachment styles.
OTHER, LESS USED APPROACHES
In their comprehensive review of the empirical literature on projective measurement of object relations, Stricker and Healey (1990) presented several instruments that had either appeared in the literature at a much earlier date and had not attracted other researchers and as a result were not used regularly, or had only recently appeared in the literature and thus required further research to assess their validity and determine the place they would take in projective object-relations measurement. Of the 10 measures that those authors reported on, only one, parental representations, has been put through the rigors of significant further empirical assessment. We will briefly present Stricker and Healey’s (1990) synopses of the nine additional measures with any research that has been conducted so as to provide a thorough presentation of projective object-relations measurement to date. We will also report on an additional approach that has not found a great deal of use thus far.
Stricker and Healey (1990) briefly mentioned three scales that were in a new developmental phase at the time of their review: The Rorschach Transitional Object Scale (Cooper, Perry, Hoke, & Richman, 1985); Phillipson’s Object Relations Technique (ORT; Phillipson, 1955), examined by Fagen and Sperling (1989); and the Affect Maturity Scale (Thompson, 1986). Although the ORT is used more widely in Great Britain, it has not yet found much of an audience in the United States. These scales have not found further evaluation since Stricker and Healey’s review.
Rorschach-Empathy-Object Relationship Scale (RE-ORS)
The Rorschach-Empathy-Object Relationship Scale (RE-ORS), developed by Pruitt and Spilka (1964), was an early attempt at assessing object-relations phenomena. Other more complex instruments have since superseded it. The development of the RE-ORS is based primarily on Rorschach theory that proposes responses of human movement and content are indicative of empathy and the capacity to relate effectively. Unlike the other Rorschach scales, therefore, this one is not derived from psychoanalytic theory. This scale uses only the human content (H) or human movement (M) response from the Rorschach data. Scale points range from 1 to 18. Higher scores represent a higher level of object relations. All scorable responses are summed and then divided by the overall number of responses in the Rorschach record. The following dimensions are tapped: Humanness, Sex Specification, Temporal-Spatial Considerations, and Movement. Reported reliability coefficients were .66 and .59.
A study of the efficacy of group therapy for vocationally handicapped–emotionally disturbed individuals was conducted using the RE-ORS assessment. Participants of group therapy scored higher than those in the control group. A significant positive correlation between RE-ORS and a measure of work adjustment emerged.
Personal Sphere Model (PSM)
Schmiedeck (1974, 1978) developed this instrument as a projective measurement of object relations. A drawing is produced that places the individual at the center and representations of others around that individual’s symbolized representation. The drawing is analyzed, providing information regarding specific object representations, the intensity of them, and perceived disruption. Sollod (1984) conducted a concurrent validity study involving college students. Level of perceived disruption was found to have a significant positive correlation with high scores on the Beck Depression Inventory and with the external dimension of Rotter’s Internal-External Locus of Control Scale. Stricker and Healey (1990) note that the PSM seems to measure interpersonal functioning as opposed to object relations.
Measurement of Symbiosis
Summers (1978) developed a procedure for scoring symbiosis in human relationships to be applied to both projective and interview data. The basis of this system appears to be more specifically derived from Mahler’s (Mahler et al., 1975) aspects of ego psychology. Summers’s system is presented in a manual in which six variables for symbiosis are identified, including undifferentiation, intrusiveness, separation difficulty, disapproval of other relationships, dependency, and injunctions. The range of reliability measures for the projective data is from 80% to 100% (using percentage of agreement) and, for the interview data, correlations range from .75 to .94. Summers and Walsh (1977) report on the system’s ability to successfully differentiate mothers of schizophrenics from mothers of normals and mothers of hospitalized nonschizophrenics. Additionally, the system differentiated schizophrenics from other patients. Stricker and Healey (1990) noted that, because Summers’s system is so specialized, it was unable to find a wide audience within the field of object-relations assessment.
Comprehensive Object Relations Profile (CORP)
The Comprehensive Object Relations Profile (CORP; Burke, Summers, Selinger, & Polonus, 1986; Summers & Burke, n.d.) measures three aspects of object relations: Object Constancy, Object Integration, and Empathy, and has two subscales: Subjectivity and Appreciation. It is a semistructured projective test in which responses are given to specific questions regarding certain interpersonal vignettes. Total score reliability was found to be .90, and median reliability for the subscales ranged from .71 to .87. Except for the two empathy subscales, discriminant validity is indicated by a lack of interscale correlations. The CORP was able to differentiate in the expected order neurotics, borderlines, and schizophrenics, thus demonstrating predictive validity. Stricker and Healey (1990) noted a strength of this measure to be it having been developed solely for object-relations assessment. They were reluctant, however, to embrace the “comprehensive” component of its title, as future research would be required to validate the manual’s claim that the dimensions tapped by the CORP are unable to be elicited from unstructured stimuli.
Since Stricker and Healey’s (1990) review, one study used the CORP to examine the relationship of God image to level of object-relations development in 92 undergraduates from a religiously homogenous population (Brokaw & Edwards, 1994). Although the objective measure of object relations that was used in the study (the Ego Function Assessment Questionnaire-Revised) correlated significantly with all three measures of God image in the predicted direction, the CORP resulted in few significant correlations.
Psychoanalytic Rorschach Profile (PRP)
The Psychoanalytic Rorschach Profile (PRP), developed by Gorlitz, Burke, and Friedman (1984; Burke, Friedman, & Gorlitz, 1988), integrates drive, ego, and object-relations theory. This instrument is comprised of 10 scales that measure impulse, ego structure, and object relations. Object-relations scales include Differentiation, Mutuality, and Animation. Higher levels of object-relations functioning are represented by higher scores on the scales. Reliability coefficients are reported to range from .59 to .88; all three object-relations scales attained coefficients of .78. Five of the seven scales, including the Differentiation scale, were able to differentiate borderline patients from schizophrenics in a pilot study. Intralevel comparisons on the Mutuality scale demonstrated high-level responses by the borderlines as compared to more evenly distributed responses by the schizophrenics.
Hansen (2000) conducted a study in which the PRP was used to assess whether human responses are necessary for a valid assessment of object relations. Results indicated that the object-relations subscales of the PRP did not discriminate between the examined diagnostic groups, including inpatients with paranoid schizophrenia or major depressive disorder, both of which are known to have distinctive patterns of object relations. The author thus concluded that the PRP object-relations scales are likely not valid measures of object relations.
Separation-Individuation Theme Scale (SITS)
Mahler’s theory of borderline development (Mahler et al., 1975) was used by Coonerty (1986) in her development of the Separation-Individuation Theme Scale (SITS). Main and additional Rorschach responses are evaluated for separationindividuation or preseparation-individuation material and subthemes of differentiation, narcissism, and rapprochement are scored. Reliabilities are reported to be between 86%, reflecting untrained raters, and 96%, reflecting trained raters. In a patient differentiation study, the scale significantly differentiated borderline from schizophrenic patients. Borderline patients were found to have a significantly higher number of separation-individuation themes and scored higher on narcissism and rapprochement subthemes.
Boundary Disturbance Scale (BDS) and Thought Disorder Scale
Based on research by Blatt and Ritzler (1974) and Blatt and Wild (1976), Lerner, Sugarman, and Barbour (1985) developed a scale for assessing boundary disturbance, a component of object relations, called the Boundary Disturbance Scale (BDS). The BDS is a 6-point, weighted scale that covers three areas, including boundary laxness, inner-outer boundary, and self-other boundary. Boundary laxness represents mild forms of ego boundary fragmentation; inner-outer boundary corresponds to more severe problems of difficulty distinguishing fantasy from reality; and self-other reflects the most severe form of boundary fragmentation and disintegration (Fowler, Hilsenroth, & Nolan, 2000). An interrater reliability coefficient of .79 is reported, with raters demonstrating 70% exact reliability and 91% agreeing within 1 point. Hospitalized patients were separated from nonhospitalized using total score and weighted scores. Hospitalized borderlines were significantly separated from all other groups based on a qualitative analysis of confabulated responses. Schizophrenic patients were separated from all other groups using contamination responses. Stricker and Healey (1990) note that the BDS provides both a refinement and extension of an aspect of objectrelations assessment.
Fowler, Hilsenroth, and Nolan (2000) conducted a study that, in part, explored the object relations of self-mutilating borderline patients. Self-mutilating borderlines were compared to non-self-mutilating borderlines. No significant differences were found between boundary laxness or inner-outer boundary disturbance. However, significant differences were found between the two groups on self-other boundary disturbance with self-mutilating borderline patients demonstrating higher incidence of self-other boundary disintegration compared to non-self-mutilating borderline patients.
Transitional Object Early Memories Probe
A newly developed assessment of an object-relations construct called the Early Memory Transitional Relatedness Scale (EMTRS) falls under the domain of early memories assessment, but in particular examines transitional object phenomenon using a specific transitional object early memories probe (Fowler, Hilsenroth, & Handler, 1998). The scale’s development is based on the assumption that a continuum exists for transitional phenomenon ranging from “pathological manifestations in which there is little or no capacity for illusion,” to “the playful, illusory use of language and objects as metaphor that constitutes healthy transitional phenomena (p. 461).” Fowler et al. (1998) found construct validity to be supported, with significant correlations between the EMTRS and therapist ratings for transitional relatedness (r ” .25, p # .03), demonstrating predictive validity of the memory probe and EMTRS. Concurrent validity was supported by a significant semipartial correlation between the Rorschach Transitional Object Scale (TOS) and the EMTRS (r ” .31, p # .02). The EMTRS scores were compared to the Rorschach Oral Dependency scores and Mutuality of Autonomy scores to demonstrate the transitional object early memory probe’s discriminant validity. None of the measures correlated with each other.
The Dietrich Object Relations and Object Representations Scale (DORORS)
The Dietrich Object Relations and Object Representations Scale (DORORS; Porcerelli & Dietrich, 1994) is a relatively new psychoanalytic object-relations scale. This scale was initially developed for use with the TAT, although the authors believe it can be applied to other projective measures. It assesses 10 specific, nonglobal aspects of internalized object relations and object representations that are partially overlapping. Each of the dimensions is scored on a 7-point scale. Higher scores correspond to higher levels of object relations. The bases for the DORORS are structural, ego psychological, and object-relations theories. Its development is rooted in clinical work and research that has dealt with parental loss, be it through death or psychiatric impairment, that results in the mother’s lack of emotional availability. Dietrich (1989) applied the DORORS to TAT data from four TAT cards in a study examining object relations and representations following the effects of early parental death. Interrater reliability within 1 point was .76. Discriminant validity was supported by the scale’s ability to differentiate participants who had lost a parent to death in contrast to those who had not for all 10 categories. Porcerelli and Dietrich (1994) reported an interrater reliability of .78 within 1 scale point. Porcerelli and Dietrich present data supporting convergent validity. A factor analysis of the DORORS resulted in the emergence of two factors. The first involves differentiation and complexity, the second aggressive derivatives and hopelessness, supporting the presence of structural and content variables. Blatt’s CORS scores correlated significantly with Factors 1 and 2 of the DORORS, and Factor 2 significantly correlated with the MOAS. Discriminant validity was supported by the lack of significant correlations between the DORORS Factor 1 and 2 and Verbal Fluency and the WAIS-R Vocabulary subtest.
CONCLUSION
Object relations are unconscious and, therefore, cannot be directly assessed. Projective measurement is the means by which we measure representations of object-relatedness. That is, we solicit information to be projected from an individual’s unconscious realm, and object-relations representations are then inferred from that dataset (Stricker & Healey, 1990). The growing body of empirical research supports both the theorized constructs that form our definition of object relations and the accuracy of our tools to measure these constructs.
Instruments reviewed in this chapter study either structural or thematic aspects of object relations. Through both components, an ideographic understanding of an individual’s intrapsychic representational world can be understood. The ability of the measures to distinguish between differing psychopathologies supports the notion that how one internalizes object relations relates to his or her level of mental health. Therefore, being able to evaluate these components of object relations is useful for both diagnostic needs and for clinical planning.
There are differing theoretical underpinnings for many of the measures as well as differing ways in which objectrelations criteria are operationalized, reflecting how the researcher has chosen to access that domain. Regardless of the theoretical legacy that has contributed to the development of the scale or of the access point by which the individual’s object relations are being viewed, the goal of all assessment is to understand how one’s intrapsychic process of internalizing others has affected how that individual constructs reality and what the consequent effect is on that individual’s internal world, including the quality of his or her mental representations, interactions, and incorporation of additional experience into his or her subjective understanding of the world (Lerner, 1998). Some researchers approach this issue in a more comprehensive manner, others in a very specialized mode. When planning assessment, it is important to be clear about the direction from which one wants to approach the question.
At the time of their review, Stricker and Healey (1990) noted the wide variety of projective approaches available to evaluate object relations, the lack of a single comprehensive system or approach to complete the task of object-relations assessment, and the likelihood that a single approach will never emerge. Considering the many dimensions of object relations and the many differing ways of conceptualizing them, it is probably more efficient to understand the question being asked and then carefully to select the tool or tools that contribute to an understanding of that question.
Research has supported the differing theoretical underpinnings of these object-relations measures and has consequently contributed to a more holistic understanding of how an individual’s object relations are formed, how they affect functioning, and from which levels they can be accessed for therapeutic intervention. Future research must continue to hone the assessment devices developed and fine-tune their ability to be sensitive to expressions of object relations. However, it must continue to look at object-relations phenomena with a flexibility that allows the contribution of other approaches to inform their continued development.
It has been more than a decade since the last review of projective measures of object relations. Since that time, there has been good news and bad news. The good news is that there continues to be a high level of promise, and projective measures, when applied in a psychometrically sound manner, appear to be capable of adding to an understanding of object relations, despite the measurement problems created by the unconscious nature of object-relations phenomena. The bad news is the paucity of additional research that has been conducted. If the promise is to be fulfilled, it will require a substantial, coordinated, and programmatic research effort, and there is little indication, outside of a handful of laboratories, that this has been undertaken. There is indication that the effort will be worthwhile, but it must be approached with a seriousness of purpose that will add luster to the efforts already undertaken.
REFERENCES
- Ackerman, S.J., Clemence, A.J., Weatherill, R., & Hilsenroth, M.J. (1999). Use of the TAT in the assessment of DSM-IV Cluster B personality disorders. Journal of Personality Assessment, 73, 422–448.
- Ackerman, S.J., Hilsenroth, M.J., Clemence, A.J., Weatherill, R., & Fowler, J.C. (2000). The effects of social cognition and object representation on psychotherapy continuation. Bulletin of the Menninger Clinic, 64, 386–408.
- Ackerman, S.J., Hilsenroth, M.J., Clemence, A.J., Weatherill, R., & Fowler, J.C. (2001). Convergent validity of Rorschach and TAT scales of object relations. Journal of Personality Assessment, 77, 295–306.
- Barends, A., Westen, D., Leigh, J., Silbert, D., & Byers, S. (1990). Assessing affect-tone of relationship paradigms from TAT and interview data. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 2, 329–332.
- Bartlett, F. (1932). Remembering: A study in experimental and social psychology. New York: Cambridge University Press.
- Berg, J.L., Packer, A., & Nunno, V.J. (1993). A Rorschach analysis: Parallel disturbance in thought and self/object representation. Journal of Personality Assessment, 61, 311–323.
- Blais, M.A., Hilsenroth, M.J., Castlebury, F., Fowler, J.C., & Baity, M.R. (2001). Predicting DSM-IV Cluster B personality disorder criteria from MMPI-2 and Rorschach data: A test of incremental validity. Journal of Personality Assessment, 76, 150–168.
- Blais, M.A., Hilsenroth, M.J., Fowler, J.C., & Conboy, C.A. (1999). A Rorschach exploration of the DSM-IV borderline personality disorder. Journal of Clinical Psychology, 55, 563–572.
462 Projective Assessment of Object Relations
- Blatt, S.J., Berman, W., Bloom-Feshbach, S., Sugarman, A., Wilber, C., & Kleber, H.D. (1984). Psychological assessment of psychopathology in opiate addicts. Journal of Nervous and Mental Disease, 172, 156–165.
- Blatt, S.J., Brenneis, C.B., Schimek, J.G., & Glick, M. (1976). Normal development and psychopathological impairment of the concept of the object on the Rorschach. Journal of Abnormal Psychology, 85, 364–373.
- Blatt, S.J., & Ford, R.Q. (1994). Therapeutic change: An object relations perspective. New York: Plenum Press.
- Blatt, S.J., Ford, R.Q., Berman, W., Cook, B., & Meyer, R. (1988). The assessment of change during the intensive treatment of borderline and schizophrenic young adults. Psychoanalytic Psychology, 5, 127–158.
- Blatt, S.J., & Lerner, H.L. (1983a). Investigations in the psychoanalytic theory of object relations and object representations. In J. Masling (Ed.), Empirical studies of psychoanalytical theories (pp. 189–249). Hillsdale, NJ: Analytic Press.
- Blatt, S.J., & Lerner, H.L. (1983b). The psychological assessment of object representation. Journal of Personality Assessment, 47, 7–28.
- Blatt, S.J., McDonald, C., Sugarman, A., & Wilber, C. (1984). Psychodynamic theories of opiate addiction: New directions for research. Clinical Psychology Review, 4, 159–189.
- Blatt, S.J., & Ritzler, B.A. (1974). Thought disorder and boundary disturbances in psychosis. Journal of Consulting and Clinical Psychology, 42, 370–381.
- Blatt, S.J., Stayner, D.A., Auerbach, J.S., & Behrends, R.S. (1996). Change in object and self-representations in long-term, intensive, inpatient treatment of seriously disturbed adolescents and young adults. Psychiatry, 59, 82–107.
- Blatt, S.J., Tuber, S.B., & Auerbach, J.S. (1990). Representation of interpersonal interactions on the Rorschach and level of psychopathology. Journal of Personality Assessment, 54, 711–728.
- Blatt, S.J., Wein, S.J., Chevron, E., & Quinlan, D.M. (1979). Parental representations and depression in normal young adults. Journal of Abnormal Psychology, 88, 388–397.
- Blatt, S.J., & Wild, C.M. (1976). Schizophrenia: A developmental analysis. New York: Academic Press.
- Blatt, S.J., Wiseman, H., Prince-Gibson, E., & Gatt, C. (1991). Object representations and change in clinical functioning. Psychotherapy, 28, 273–283.
- Bornstein, R.F., Galley, D.J., & Leone, D.R. (1986). Parental representations and orality. Journal of Personality Assessment, 50, 80–89.
- Brokaw, B.F., & Edwards, K.J. (1994). The relationship of God image to level of object relations development. Journal of Psychology and Theology, 22, 352–371.
- Burke, W.F., Friedman, G., & Gorlitz, P. (1988). The Psychoanalytic Rorschach Profile: An integration of drive, ego, and object relations perspectives. Psychoanalytic Psychology, 5, 193–212.
- Burke, W.F., Summers, F., Selinger, D., & Polonus, T.W. (1986). The Comprehensive Object Relations Profile: A preliminary report. Psychoanalytic Psychology, 3, 173–185.
- Cogan, R., & Porcerelli, J.H. (1996). Object relations in abusive partner relationships: An empirical investigation. Journal of Personality Assessment, 66, 106–115.
- Conklin, A., & Westen, D. (2001). Thematic Apperception Test. In W.I. Dorfman & M. Hersen, (Eds.), Understanding psychological assessment: Perspectives on individual differences. (pp. 107– 133). New York: Kluwer/Plenum.
- Cook, B., Blatt, S.J., & Ford, R.Q. (1995). The prediction of therapeutic response of long-term intensive treatment of seriously disturbed young adult inpatients. Psychotherapy Research, 5, 218–230.
- Coonerty, S. (1986). An exploration of separation-individuation themes in the borderline personality disorder. Journal of Personality Assessment, 50, 501–512.
- Cooper, S.H., Perry, J.C., Hoke, L., & Richman, N. (1985). Transitional relatedness and borderline personality disorder. Psychoanalytic Psychology, 2, 115–128.
- Derogatis, L.R. (1977). SCL-90: Administration, scoring, and procedures manual-1 for the R version. Baltimore: Author.
- Diamond, D., Blatt, S.J., Stayner, D., & Kaslow, N. (1991). Selfother differentiation of object representations. Unpublished research manual, Yale University, New Haven, CT.
- Dietrich, D.R. (1989). Early childhood parent death, psychic trauma and organization, and object relations. In D.R. Dietrich & P.C. Shabad (Eds.), The problem of loss and mourning: Psychoanalytic perspectives (pp. 277–335). Madison, CT: International Universities Press.
- Fagen, G., & Sperling, M.B. (1989, April). The research utility of the Object Relations Technique for assessing attachment and relational defenses. Paper presented at the meeting of the Society for Personality Assessment, New York.
- Farris, M.A. (1988). Differential diagnosis of borderline and narcissistic personality disorders. In H.D. Lerner & P.M. Lerner (Eds.), Primitive mental states and the Rorschach (pp. 299– 337). Madison, CT: International Universities Press.
- Fowler, C., Hilsenroth, M.J., & Handler, L. (1995). Early memories: An exploration of theoretically derived queries and their clinical utility. Bulletin of the Menninger Clinic, 59, 79–98.
- Fowler, C., Hilsenroth, M.J., & Handler, L. (1996a). A multimethod approach to assessing dependency: The Early Memory Dependency Probe. Journal of Personality Assessment, 67, 399–413.
- Fowler, C., Hilsenroth, M.J., & Handler, L. (1996b). Two methods of early memories data collection: An empirical comparison of the projective yield. Assessment, 3, 63–71.
- Fowler, C., Hilsenroth, M.J., & Handler, L. (1998). Assessing transitional phenomena with the transitional object memory probe. Bulletin of the Menninger Clinic, 62, 455–473.
- Fowler, C., Hilsenroth, M.J., & Handler, L. (2000). Martin Mayman’s Early Memories Technique: Bridging the gap between personality
assessment and psychotherapy. Journal of Personality Assessment, 75, 18–32.
- Fowler, J.C., Hilsenroth, M.J., & Nolan, E. (2000). Exploring the inner world of self-mutilating borderline patients: A Rorschach investigation. Bulletin of the Menninger Clinic, 64, 365–385.
- Frieswyk, S., & Colson, D. (1980). Prognostic considerations in the hospital treatment of borderline states: The perspective of object relations theory and the Rorschach. In J.S. Kwawer, H.D. Lerner, P.M. Lerner, & A. Sugarman (Eds.), Borderline phenomena and the Rorschach test (pp. 229–255). New York: International Universities Press.
- Gorlitz, P., Burke, W., & Friedman, G. (1984). Manual for the Psychoanalytic Rorschach Profile. Unpublished manuscript.
- Hansen, J.T. (2000). Human responses in assessing object relations subscales of the Psychoanalytic Rorschach Profile. Psychological Reports, 87, 675–676.
- Harder, D.W., Greenwald, D.F., Wechsler, S., & Ritzler, B.A. (1984). The Urist Rorschach Mutuality of Autonomy Scale as an indicator of psychopathology. Journal of Clinical Psychology, 40, 1078–1083.
- Hatcher, R.L., & Krohn, A. (1980). Level of object representation and capacity for intensive psychotherapy in neurotics and borderlines. In J.S. Kwawer, H.D. Lerner, P.M. Lerner, & A. Sugarman (Eds.), Borderline phenomena and the Rorschach test (pp. 299– 320). New York: International Universities Press.
- Hernandez, N.A., Hinrichsen, G.A., & Lapidus, L.B. (1998). An empirical study of object relations in adult children of depressed elderly mothers. International Journal of Aging and Human Development, 46, 143–156.
- Hibbard, S., Hilsenroth, M.J., Hibbard, J.K., & Nash, M.R. (1995). A validity study of two projective object representation measures. Psychological Assessment, 7, 432–439.
- Holaday, M., & Sparks, C.L. (2001). Revised guidelines for Urist’s Mutuality of Autonomy Scale (MOA). Assessment, 8, 145–155.
- Kavanagh, G.G. (1985). Changes in patients’ object representations during psychoanalysis and psychoanalytic psychotherapy. Bulletin of the Menninger Clinic, 49, 546–564.
- Kern, C., & Roll, S. (2001). Object representations in dreams of Chicanos and Anglos. Dreaming: Journal of the Association for the Study of Dreams, 11, 149–166.
- Kernberg, O. (1966). Structural derivatives of object relationships. International Journal of Psycho-analysis, 47, 236–253.
- Kernberg, O. (1975). Borderline conditions and pathological narcissism. New York: Jason Aronson.
- Kernberg, O. (1977). The structural diagnosis of borderline personality organization. In P. Harticollis (Ed.), Borderline personality disorders (pp. 87–122). New York: International Universities Press.
- Kohut, H. (1966). Forms and transformations of narcissism. Journal of the American Psychoanalytic Association, 14, 243–272.
- Kohut, H. (1971). The analysis of the self. New York: International Universities Press.
- Kohut, H. (1977). The restoration of the self. New York: International Universities Press.
- Krohn, A., & Mayman, M. (1974). Object representations in dreams and projective tests. Bulletin of the Menninger Clinic, 38, 445– 466.
- Last, J.M. (1983). Comprehensive early memory scoring system manual. Unpublished manuscript.
- Last, J.M., & Bruhn, A.R. (1983). The psychodiagnostic value of children’s earliest memories. Journal of Personality Assessment, 47, 597–603.
- Last, J.M., & Bruhn, A.R. (1985). Distinguishing child diagnostic types with early memories. Journal of Personality Assessment, 49, 187–192.
- Leigh, J., Westen, D., Barends, A., Mendel, M., & Byers, S. (1992). The assessment of complexity of representations of people using TAT and interview data. Journal of Personality, 60, 809–837.
- Lerner, H.D., & St. Peter, S. (1984a). Patterns of object relations in neurotic, borderline and schizophrenic patients. Psychiatry, 47, 77–92.
- Lerner, H.D., & St. Peter, S. (1984b). The Rorschach H response and object relations. Journal of Personality Assessment, 48, 345–350.
- Lerner, H.D., Sugarman, A., & Barbour, C.G. (1985). Patterns of ego boundary disturbance in neurotic, borderline, and schizophrenic patients. Psychoanalytic Psychology, 2, 47–66.
- Lerner, P.M. (1998). Psychoanalytic perspectives on the Rorschach. Hillsdale, NJ: Analytic Press.
- Levine, L.V., & Tuber, S.B. (1993). Measures of mental representation: Clinical and theoretical considerations. Bulletin of the Menninger Clinic, 57, 69–87.
- Levine, L.V., Tuber, S.B., Slade, A., & Ward, M.J. (1991). Mothers’ mental representations and their relationship to mother-infant attachment. Bulletin of the Menninger Clinic, 55, 454–469.
- Levy, K.N., Blatt, S.J., & Shaver, P.R. (1998). Attachment styles and parental representation. Journal of Personality and Social Psychology, 74, 407–419.
- Mahler, M., Pine, F., & Bergman, A. (1975). The psychological birth of the human infant. New York: Basic Books.
- Malinoski, P., Lynn, S.J., & Sivec, H. (1998). The assessment, validity, and determinants of early memory reports: A critical review. In S.J. Lynn & K.M. McConkey (Eds.), Truth in memory (pp. 109–136). New York: Guilford Press.
- Mayman, M. (1967). Object-representations and object-relationships in Rorschach responses. Journal of Projective Techniques and Personality Assessment, 31, 17–24.
- Mayman, M. (1968). Early memories and character structure. Journal of Projective Techniques and Personality Assessment, 32, 303–316.
- Mayman, M., & Faris, M. (1960). Early memories as expressions of relationship paradigms. American Journal of Orthopsychiatry, 30, 507–520.
464 Projective Assessment of Object Relations
- Murray, J.F. (1985). Borderline manifestations in the Rorschachs of male transsexuals. Journal of Personality Assessment, 49, 454– 466.
- Nigg, J.T., Lohr, N.E., Westen, D., Gold, L.J., & Silk, K.R. (1991). Malevolent object representations in borderline personality disorder and major depression. Journal of Abnormal Psychology, 101, 61–67.
- Nigg, J.T., Silk, K.R., Westen, D., Lohr, N.E., Gold, L.J., Goodrich, S., et al. (1992). Object representations in the early memories of sexually abused borderline patients. American Journal of Psychiatry, 148, 864–869.
- Phillipson, H. (1955). The Object Relations Technique. Glencoe, IL: Free Press.
- Piaget, J. (1956). The construction of reality in the child. New York: Basic Books.
- Piran, N. (1988). Borderline phenomena in anorexia nervosa and bulimia. In H.D. Lerner & P.M. Lerner (Eds.), Primitive mental states and the Rorschach (pp. 363–376). Madison, CT: International Universities Press.
- Piran, N., & Lerner, P.M. (1988). Rorschach assessment of anorexia nervosa and bulimia. In C.D. Spielberger & J.N. Butcher (Eds.), Advances in personality assessment (pp. 77–101). Hillsdale, NJ: Erlbaum.
- Porcerelli, J.H., Cogan, R., & Hibbard, S. (1998). Cognitive and affective representations of people and MCMI-II personality psychopathology. Journal of Personality Assessment, 70, 535– 540.
- Porcerelli, J.H., & Dietrich, D.R. (1994). Dietrich Object Relations and Object Representations Scale: Convergent and discriminant validity and factor structure. Psychoanalytic Psychology, 11, 101–113.
- Porcerelli, J.H., Hill, K.A., & Dauphin, V.B. (1995). Needgratifying object relations and psychopathology. Bulletin of the Menninger Clinic, 59, 99–105.
- Pruitt, W.A., & Spilka, B. (1964). Rorschach Empathy-Object Relationship Scale. Journal of Projective Techniques and Personality Assessment, 28, 331–336.
- Quinlan, D.M., Blatt, S.J., Chevron, E.S., & Wein, S.J. (1992). The analysis of descriptions of parents: Identification of a more differentiated factor structure. Journal of Personality Assessment, 59, 340–351.
- Ritzler, B., Zambianco, D., Harder, D., & Kaskey, M. (1980). Psychotic patterns of the concept of the object on the Rorschach test. Journal of Abnormal Psychology, 89, 46–55.
- Ryan, E.R. (1974). Quality of object relations scale. Unpublished manuscript.
- Ryan, E.R., & Bell, M.D. (1984). Changes in object relations from psychosis to recovery. Journal of Abnormal Psychology, 93, 209–215.
- Ryan, E.R., & Cicchetti, D.V. (1985). Predicting quality of alliance in the initial psychotherapy interview. Journal of Nervous and Mental Disease, 173, 717–725.
- Schmiedeck, R. (1974). The Personal Sphere Model: A new projective tool. Bulletin of the Menninger Clinic, 38, 113–128.
- Schmiedeck, R. (1978). The Personal Sphere Model. New York: Grune & Stratton.
- Schwager, E., & Spear, W.E. (1981). New perspectives on psychological tests as measures of change. Bulletin of the Menninger Clinic, 45, 527–541.
- Segal, H.G., Westen, D., Lohr, N.E., & Silk, K.R. (1993). Clinical assessment of object relations and social cognition using stories told to the Picture Arrangement subtest of the WAIS-R. Journal of Personality Assessment, 61, 58–80.
- Segal, H.G., Westen, D., Lohr, N.E., Silk, K., & Cohen, R. (1992). Assessing object relations and social cognition in borderline personality disorders from stories told to the Picture Arrangement subtest of the WAIS-R. Journal of Personality Disorders, 6, 458–470.
- Sollod, R.N. (1984). The Personal Sphere Model: Psychometric properties and concurrent validity in a college population. Psychological Reports, 55, 727–736.
- Spear, W.E. (1980). The psychological assessment of structural and thematic object representations in borderline and schizophrenic patients. In J.S. Kwawer, H.D. Lerner, P.M. Lerner, & A. Sugarman (Eds.), Borderline phenomena and the Rorschach test (pp. 321–340). New York: International Universities Press.
- Spear, W.E., & Sugarman, A. (1984). Dimensions of internalized object relations in borderline and schizophrenic patients. Psychoanalytic Psychology, 1, 113–129.
- Stayner, D. (1994). The relationship between clinical functioning and changes in self and object representations in the treatment of severely impaired inpatients. Unpublished doctoral dissertation, Teacher’s College, Columbia University, New York, NY.
- Strauss, J., & Ryan, R.M. (1987). Autonomy disturbances in subtypes of anorexia nervosa. Journal of Abnormal Psychology, 96, 254–258.
- Stricker, G., & Gold, J.R. (1999). The Rorschach: Toward a nomothetically based, idiographically applicable configurational model. Psychological Assessment, 11, 240–250.
- Stricker, G., & Healey, B.J. (1990). Projective assessment of object relations: A review of the empirical literature. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 2, 219–230.
- Stuart, J., Westen, D., Lohr, N., Benjamin, J., Becker, S., Vorus, N., et al. (1990). Object relations in borderlines, depressives, and normals: An examination of human responses on the Rorschach. Journal of Personality Assessment, 55, 296–318.
- Summers, F. (1978). Manual for the measurement of symbiosis in human relationships. Psychological Reports, 43, 663–670.
- Summers, F., & Burke, W.F. (n.d.). Comprehensive Object Relations Profile. Unpublished manuscript.
- Summers, F., & Walsh, F. (1977). The nature of the symbiotic bond between mother and schizophrenic. American Journal of Orthopsychiatry, 47, 484–494.
- Thompson, A.E. (1986). An object relational theory of affect maturity: Applications to the Thematic Apperception Test. In M. Kissen (Ed.), Assessing object relations phenomena (pp. 207– 224). Madison, CT: International Universities Press.
- Tuber, S.B. (1983). Children’s Rorschach scores as predictors of later adjustment. Journal of Consulting and Clinical Psychology, 51, 379–385.
- Urist, J. (1977). The Rorschach test and the assessment of object relations. Journal of Personality Assessment, 41, 3–9.
- Urist, J. (1980). Object relations. In R.H. Woody (Ed.), Encyclopedia of clinical assessment (Vol. 1, pp. 821–833). San Francisco: Jossey-Bass.
- Urist, J., & Schill, M. (1982). Validity of the Rorschach Mutuality of Autonomy Scale: A replication using excerpted responses. Journal of Personality Assessment, 46, 450–454.
- Werner, H. (1948). Comparative psychology of mental development. New York: International Universities Press.
- Westen, D. (1985/1989). Object relations and social cognition TAT scoring manual. Unpublished manuscript, University of Michigan, Ann Arbor.
- Westen, D. (1991a). Clinical assessment of object relations using the TAT. Journal of Personality Assessment, 56, 56–74.
- Westen, D. (1991b). Social cognition and object relations. Psychological Bulletin, 109, 429–455.
- Westen, D., Huebner, D., Lifton, N., & Silverman, M. (1991). Assessing complexity of representations of people and understanding of social causality: A comparison of natural science and clinical psychology graduate students. Journal of Social and Clinical Psychology, 10, 448–458.
- Westen, D., Lohr, N., Silk, K.R., Gold, L., & Kerber, K. (1990). Object relations and social cognition in borderlines, major depressives, and normals: A Thematic Apperception Test analysis. Psychological Assessment: A Journal of Consulting and Clinical Psychology, 2, 355–364.
Projective Assessment of Defense Mechanisms
JOHN H. PORCERELLI AND STEPHEN HIBBARD
Rorschach Responses 468
THEORY OF DEFENSE MECHANISMS 466 DEFENSE MECHANISMS AND PSYCHOPATHOLOGY 467 DEFENSE MECHANISMS SCALES FOR PROJECTIVE TESTS 468 Lerner Defense Scale (LDS) for the Assessment of Human
The concept of ego defense mechanisms has lasted the test of time and has lent important information to the study of normal development, adaptation, and psychopathology (Porcerelli, Thomas, Hibbard, & Cogan, 1998). Increasing empirical support for the validity of defenses over the past decade has led to the inclusion of a provisional axis for defensive functioning (Perry et al., 1998) in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV; American Psychiatric Association, 1994). Currently, there are a variety of methods to assess defenses including self-report scales, rating scales for clinical interview and psychotherapy sessions, and scales for projective test data. A comprehensive review of these methods can be found in Cramer (1991b), a special issue of the Journal of Personality (Cramer & Davison, 1998), Perry (1993), and Vaillant (1992).
This chapter will focus on the projective assessment of defense mechanisms. Of the many scales available, the authors have chosen three for review, utilizing two methods of projective assessment: the Rorschach (Rorschach, 1942) and the Thematic Apperception Test (Murray, 1943). These assessment methods have been selected because they have received reasonable empirical validation and they are a part of (or could be included within) a comprehensive psychological test battery. This chapter will include sections on the theory of defense mechanisms, the relationship between defenses and psychopathology, a review of three defense scales (including a description of each scale, reliability and validity, strengths and limitations, and cross-cultural studies), and a conclusion.
Rorschach Defense Scales (RDS) for Assessing the Content of Rorschach Responses 469 Defense Mechanism Manual (DMM) for the Assessment of Thematic Apperception Test Stories 470 SUMMARY AND CONCLUSIONS 472 REFERENCES 473
THEORY OF DEFENSE MECHANISMS
The concept of defense mechanisms was introduced by Sigmund Freud in his 1894 paper “The Neuro-Psychoses of Defense.” He conceptualized defenses as mental forces that opposed unacceptable ideas or feelings that, if acknowledged, would cause significant distress. Freud viewed specific defenses as characteristics of certain symptoms and psychological conditions. Obsessional neurosis was associated with the defense of displacement, hysteria with the defense of conversion, and paranoia (Freud, 1896) with the defense of projection. With the introduction of the structural theory (Freud, 1923) and the theory of signal anxiety (Freud, 1926), Freud placed the concept of defense within the heart of psychoanalytic theory. Defenses were viewed as functions of the ego that protected the individual from anxiety associated with external (e.g., parents) and internal (e.g., guilt from the superego) dangers. These developmentally sequenced dangers include loss of the object, loss of the object’s love, fear of castration, and fear of condemnation from the superego. When an unacceptable idea or wish threatened to enter consciousness and thus elicit anxiety associated with the aforementioned dangers, an unconscious process was set in motion by a modicum of anxiety that signaled the need for defenses. Anna Freud (1936) refined and extended the concept of defense mechanisms and developed a classification system based upon the various types of anxieties that were defended against. Her list included repression, regression, reaction formation, displacement, projection, isolation, undoing, denial, turning against the self, and reversal.
As the theory of ego psychology expanded, so did the concept of defense. Brenner (1955, 1982), emphasizing the adaptive and accommodating role of the ego, veered from discrete defense mechanisms and put forth the notion that anything that the ego uses to reduce anxiety or depressive affect could be considered a defense. Schafer (1968) articulated how defenses could block expression of unacceptable thoughts or feelings and at the same time express, in disguised form, that which is unacceptable. For example, when aggressive feelings are projected onto another, the individual using the defense blocks the awareness of the ownership of the feelings but is able to experience the aggression as coming from the other and covertly gratify aggressive wishes.
Object-relations theorists offered elaborations of the concept of defense mechanisms. Through her experiences working with children and severely disturbed adults, Klein (1946) described the defenses of splitting, idealization, introjection, omnipotence, and projective identification. These defenses involve distortions of self- and object representations as a function of inner tensions and impulses. Winnicott (1965) added to the classical notion of defense by describing how traumatic failures on the part of early caregivers can result in a defensively constructed “false self” in order to protect self-esteem. Modell (1975) rejected the classical theory that defenses were only constructed against id impulses and suggested that defenses can be brought about through severe empathic failures. He introduced the defense of “self-sufficiency” to describe the turning away from important caregivers in order to avoid overwhelming negative affects associated with empathic failures. From a self-psychological perspective, Kohut (1984) also spoke of defenses as being organized around empathic failures in order to protect a vulnerable or “enfeebled” self.
Kernberg (1967, 1975, 1984) contributed to the understanding of defensive structures in borderline personality organization. Drawing from both structural and object-relations theories, Kernberg identified levels of personality organization—neurotic, borderline, psychotic—and the clusters of defenses that predominated within each level. Unlike the neurotic level, where defenses are organized around repression and related defenses, the borderline personality organization is identified by the defense of splitting and related defenses (devaluation, idealization, omnipotence, denial, and projective identification). Splitting refers to the psychic splitting of self- and object representations into “all-good” and “all-bad.” It is the all-bad images that are psychologically split off in order to preserve positive aspects of self and other. At the psychotic level, splitting and other primitive defenses (e.g., massive denial) are used to “protect the patient from total loss of ego boundaries and dreaded fusion experiences with
others which reflect their lack of differentiation of self and object images” (Kernberg, 1984, p. 179).
DEFENSE MECHANISMS AND PSYCHOPATHOLOGY
Defense mechanisms are associated with adaptive as well as psychopathological functioning (Vaillant, 1976, 1977, 1993). Defenses can be conceptualized along a developmental continuum from immature to mature. Immature defenses arise early in life and thus are cognitively less complex (e.g., denial). Mature defenses (e.g., sublimation) become prominent in late adolescence and adulthood when mental processes become more differentiated and complex. If an adult continues to rely on an age-inappropriate defense, it would be considered “pathological” or “primitive.” Vaillant (1971, 1977) conceptualized a hierarchy of defenses within each individual. That is, every person has a repertoire of mature and immature defenses at their disposal. Psychologically healthy individuals exhibit a greater relative use of adaptive defenses (altruism, suppression, humor, and sublimation) than, for example, major image-distorting defenses (autistic fantasy, projective identification, splitting), commonly seen in Cluster B personality disorders. Comparatively, individuals suffering from borderline personality disorder are likely to use higher percentages of major image-distorting defenses and lower percentages of adaptive defenses (Bond, Paris, & Zweig-Frank, 1994; Devens & Erickson, 1998).
There are several issues to take into account when determining whether a defense or cluster of defenses is pathological. One must consider the age of the person using the defense, the context within which the defense occurs, the persistence of its use, and the type of defense used. With regard to age, one would expect a 5-year-old to use blatant denial, but not a mature, relatively intelligent adult. However, the issue of context may come into play. What if an adult has just been diagnosed with a malignant brain tumor? The use of blatant denial (i.e., “I don’t have a brain tumor!”) may well be adaptive and may temporarily shield the person from experiencing overwhelming anxiety, especially if the person is eventually able to accept the reality of his or her condition and make appropriate decisions regarding treatment. Considering the issue of persistence of use, if this same person continues to deny the diagnosis of cancer, his or her ability to adaptively deal with the condition will be severely affected and most clinicians (and loved ones) would agree that the defense has become pathological. Willick (1995) states that defenses are pathological “only when they are utilized so rigidly and persistently that they become the most prominent feature of the structure of the pathological symptom, character trait, or personality organization” (p. 487). An example would be the developmentally immature defense of splitting in patients with borderline personality disorder. The splitting of objects (object representations) into all-good and all-bad is a hallmark of the disorder. It is not being suggested that immature defenses such as splitting are never used by healthy or neurotic individuals. They would just be low on the defense hierarchy of healthier people.
DEFENSE MECHANISMS SCALES FOR PROJECTIVE TESTS
In the 1980s, two formal scoring manuals were developed for Rorschach responses—the Lerner Defense Scale (LDS; Lerner & Lerner, 1980) and the Rorschach Defense Scales (RDS; Cooper, Perry, & Arnow, 1988). A formal scoring manual for Thematic Apperception Test responses—the Defense Mechanism Manual (DMM; Cramer, 1991b)—was developed in the late 1980s but has become the most frequently used projective measure of defense. These three scoring systems will be described in detail.
Lerner Defense Scale (LDS) for the Assessment of Human Rorschach Responses
Theoretical Foundation and Description
The Lerner Defense Scale (LDS) draws upon the theoretical conceptualizations of Kernberg (1975, 1976) regarding object relations and defensive organization of borderline patients. These scales do not code for the occurrence of more adaptive or more neurotic defenses. Lerner and Lerner were also influenced by Mayman (1967), Pruitt and Spilka (1964), and Holt (1970) in the development of the scales. In particular, they were influenced by Mayman’s object-relational perspective on the Rorschach and Holt’s well-known efforts to describe Rorschach responses in terms of drive and defense sequencing. The Lerner and Lerner scale is made up of the five defenses characteristic of borderline personality organization and is applied only to Rorschach human responses. Only human responses are coded because of the theoretical connection between object relations and defense (Lerner, 1990).
Operationalized Defenses
The LDS scoring manual includes five defenses.
- Splitting: Includes one level.
- Devaluation: Includes five levels ranging from Level 1 (minor devaluation of a human figure) to Level 5 (loss of the humanness of a figure).
- Idealization: Includes five levels ranging from Level 1 (a human figure described in a mildly positive way) to Level 5 (highly idealized, nonhuman figure).
- Projective Identification: Includes one level.
- Denial: Includes three levels ranging from Level 1 (negation, intellectualization, minimization, repudiation) to Level 3 (a spoiled response—something is added to the blot that is not there or an obvious aspect of the blot is not taken into account).
Higher levels of devaluation, idealization, and denial defenses indicate more pathological versions of the defense.
Reliability
Interrater reliability has ranged from 83% to 100% exact agreement for the five major defense categories and from 76% to 95% exact agreement for the subcategories of idealization, devaluation, and denial (Lerner & Lerner, 1980). Gacono, Meloy, and Berg (1992) reported 100% agreement for three of five of the major LDS categories. Interrater reliability could not be calculated for splitting and projective identification due to a lack of responses in a sample of individuals diagnosed with narcissistic, borderline, and antisocial personality disorder. All other investigations have reported similarly high levels of interrater reliability (Gacono, 1990; Hilsenroth, Hibbard, Nash, & Handler, 1993; Lerner & Van-Der Keshet, 1995; Pinheiro, Sousa, Da Silva, Horta, De Souza, & Fleming, 2001). No other types of reliability data have been reported for the LDS.
Validity
The majority of studies with the LDS have compared borderline patients with other diagnostic groups. Lerner and Lerner (1980) compared outpatients diagnosed with borderline personality disorder and patients diagnosed with neurotic disorders. Patients in the borderline personality disorder group used more splitting, low-level devaluation, projective identification, and high-level denial than patients within the neurotic group. Patients within the neurotic group used more high-level devaluation, high-level denial, and idealization than patients within the borderline group. In comparing hospitalized patients, Lerner, Sugarman and Gaughran (1981) reported more splitting, devaluation, and projective identification in patients diagnosed with borderline personality disorder than in patients diagnosed with schizophrenia. These findings seemed to call into question Kernberg’s (1975) conceptualization that borderline and schizophrenic patients share similar primitive defenses and/or the ability of the LDS to accurately assess defensive functioning in patients with schizophrenia. The lack of human percepts produced by schizophrenic patients may limit the scale’s usefulness with that population. However, in the study of patients diagnosed with narcissistic, borderline, and antisocial personality disorders, Gacono et al. (1992) were unable to compare LDS scores because of too few human responses offered by their sample. In an earlier study by Gacono (1990), the LDS failed to differentiate patients diagnosed with antisocial personality disorder with severe and moderate psychopathy as defined by the Psychopathy Checklist Revised (Hare, 1985). Hilsenroth et al. (1993) compared patients diagnosed with narcissistic, borderline, and Cluster C personality disorders using the LDS and other measures of personality functioning. They reported that patients with borderline personality disorder used more primitive defenses than patients diagnosed with Cluster C personality disorders and used more splitting and projective identification than patients with narcissistic personality disorder. Patients with narcissistic personality disorders used more idealization than patients with Cluster C personality disorders. In addition, correlations between LDS scores and a measure of primitive aggression by Holt (1977) supported the convergent and discriminant validity for the LDS. In a large-scale study involving 134 family triads (father-motherson, N ” 402) that tested the relationship between identification between fathers and sons and cocaine addiction in adolescents, Pinheiro et al. (2001) reported greater use of splitting, projective identification, low-level denial, moderatelevel idealization, and moderate- and low-level devaluation by adolescents diagnosed with a cocaine addiction than nonaddicted controls. Fathers of adolescent sons with cocaine addictions used more splitting, projective identification, low-level denial, moderate- and low-level idealization, and moderate- and low-level devaluation than fathers of nonaddicted adolescent controls. Mothers of adolescent sons diagnosed with cocaine addictions used more projective identification, low-level denial, moderate-level idealization, and moderate- and low-level devaluation than mothers of nonaddicted adolescent controls. In a study comparing ballet students with patients with eating disorders, Lerner and Van-Der Keshet (1995) found that patients with anorexia (restrictive and bulimic types) and ballet students with anorexic symptoms used splitting and devaluation significantly more than asymptomatic ballet students and normal controls. Anorexic (restrictive type) patients used significantly more denial than all other groups. Problematic, however, was the finding that normal controls used significantly more idealization than all
other groups. This finding is consistent with Lerner and Lerner (1980), who found significantly greater idealization scores in patients classified as neurotic as opposed to patients in a borderline personality disorder group. Lerner and Van-Der Keshet (1995) suggest that the upper ratings of the idealization category (Level 1 and 2) may be more sensitive to adaptive aspects of the defense and that none of the five levels assess primitive aspects of idealization. These findings call into question the inclusion of idealization in the LDS.
Cross-Cultural Studies
No available studies.
Strengths
The LDS is solidly grounded in psychodynamic theory of personality organization and has demonstrated consistently high levels of interrater reliability. Four of six studies appear to support the scale’s ability to identify borderline functioning and differentiate borderline personality disorder and more and less severe groups.
Limitations
The LDS offers a limited range of defenses and thus restricts its use to patients diagnosed with personality pathology and other severe disturbances. For research and clinical uses, a limited range of defenses does not provide important information on the coexistence of healthier, more adaptive defenses (i.e., patient strengths). Lerner, Albert, and Walsh (1987) reported high intercorrelations for four of five defenses, with the correlations between splitting and projective identification reaching .76. Such high intercorrelations can cut down on the psychometric properties of the overall scale. The LDS’s reliance on human responses is likely to limit information about psychotic-level defenses and in some samples of patients with personality disorders (e.g., Gacono et al., 1992). Use of the LDS requires highly specific training for administration (of the Rorschach) and interpretation.
Rorschach Defense Scales (RDS) for Assessing the Content of Rorschach Responses
Theoretical Foundation and Description
The Rorschach Defense Scales (RDS) draw from the theoretical developments of Winnicott (1953), Kernberg (1975), Kohut (1977), and Stolorow and Lachman (1980) and the assessment contributions of Schafer (1954), Holt (1960), Weiner (1966), Lerner and Lerner (1980), and Sugarman (1980) for the development of scoring criteria. The RDS includes 15 defenses, each of which contains from 6 to 14 scoring categories (132 scoring criteria). A broad range of defenses were chosen to assess prestage defenses of patients with structural deficiencies as well as those with more advanced ego development. Scoring categories rely heavily on the content of Rorschach responses (human and nonhuman percepts) and secondarily on formal scores and examinerpatient interactions.
Operationalized Defenses
The RDS scoring manual includes three levels of defenses representing neurotic, borderline, and psychotic levels of personality organization.
- Neurotic defenses: Includes higher level denial, isolation, intellectualization, reaction formation, rationalization, Pollyannaish denial, and repression.
- Borderline defenses: Includes devaluation, primitive idealization, projective identification, splitting, omnipotence, and projection.
- Major distortion defenses: Includes massive denial and hypomanic denial.
Reliability
Cooper, Perry, and Arnow (1988) reported interrater reliability (intraclass) coefficients of .71, .81, and .72, for the neurotic, borderline, and psychotic categories, respectively. Lerner et al. (1987) reported 64% exact agreement for the aggregate of all RDS defenses. No other types of reliability data have been reported for the RDS.
Validity
Cooper et al. (1988) reported an association between borderline psychopathology and the use of devaluation, projection, splitting, and hypomanic denial. Intellectualization and isolation (obsessional defenses) were negatively associated with patients with borderline functioning and positively associated with bipolar II affective disorder patients. Interestingly, no associations were found between antisocial personality symptoms and RDS scores. Lerner et al. (1987) reported higher scores on splitting, devaluation, and omnipotence in patients with borderline personality disorder as compared to the patients diagnosed with schizophrenia and neurotic disorders. Significant correlations were reported between LDS and RDS for splitting and devaluation, supporting convergent validity for those defenses. Gacono et al. (1992) reported greater use of idealization in patients with narcissistic and borderline personality disorders than in patients with antisocial personality disorder. Antisocial personality disorder patients who met criteria for psychopathy scored consistently higher on massive denial, splitting, projective identification, omnipotence, and devaluation than patients with nonpsychopathic personality disorders. However, the differences did not meet statistical significance. In a follow-up study of Cooper’s (Cooper et al., 1988) original validity study for the RDS, Cooper, Perry, and O’Connell (1991) assessed the predictive value of the RDS in relation to symptoms and psychosocial functioning. Significant correlations were reported between devaluation and projection and affective symptoms and social relationships. Several neurotic-level defenses (intellectualization, isolation, reaction-formation, and Pollyannaish denial) were associated with fewer symptoms and better social functioning.
Cross-Cultural Studies
No available studies.
Strengths
RDS is solidly grounded in psychoanalytic theories of defense. The RDS covers a wide range of personality functioning from primitive defenses to more mature and adaptive defenses as well as assesses defense clusters associated with certain character styles (e.g., obsessional). Adequate interrater reliability has been reported both within and outside Cooper’s lab. As with the LDS, certain RDS defenses have been able to identify borderline functioning and differentiate borderline personality disorder from more and less severe levels of psychopathology. In addition, certain RDS defenses were able to predict affective symptoms and social functioning at follow-up (approximately 2 years).
Limitations
Use of the RDS requires highly specific training for administration and interpretation. The RDS has been reported in far fewer validity studies than any of the other scales.
Defense Mechanism Manual (DMM) for the Assessment of Thematic Apperception Test Stories
Theoretical Foundation and Description
The DMM combines psychoanalytic ego psychology and cognitive developmental approaches to assess three defenses. Each defense includes seven categories (21 scoring criteria). Each of the three defenses can also be subdivided into mature and immature levels.
Operationalized Defenses
The DMM scoring manual includes denial, projection, and identification. These defenses are conceptualized as occurring on a developmental hierarchy, with denial being most prominent in childhood, projection being most prominent in preadolescence, and identification being most prominent in late adolescence and adulthood.
Categories for denial include:
- D1—Omission of major characters or objects.
- D2—Misperception.
- D3—Reversal.
- D4—Negation.
- D5—Denial of reality.
- D6—Overly maximizing the positive or minimizing the negative.
- D7—Unexpected goodness, optimism, positiveness, or gentleness.
Categories for projection include:
- P1—Attribution of hostile feelings or intentions, or other normatively unusual feelings or intentions, to a character.
- P2—Additions of ominous people, animals, objects, or qualities.
- P3—Magical or autistic thinking.
- P4—Concern for protection from external threat.
- P5—Apprehensiveness of death, injury, or assault.
- P6—Themes of pursuit, entrapment, and escape.
- P7—Bizarre story or theme.
Categories for identification include:
- I1—Emulation of skills.
- I2—Emulation of characteristics, qualities, or attitudes.
- I3—Regulation of motives or behavior.
- I4—Self-esteem through affiliation.
- I5—Work and delay of gratification.
- I6—Role differentiation.
- I7—Moralism.
The first five levels of denial, the first three levels of projection, and the first two levels of identification are considered immature subscales of their parent scales.
Reliability
Interrater reliability (Pearson) coefficients have ranged between .56 and .80 for denial, .71 and .91 for projection, and .59 and .89 for identification and from .81 to .93 when interrater reliability is reported as a total defense (i.e., an aggregate of all three defenses) score (Cramer, 1991a, 1991b, 1997a, 1999; Cramer, Blatt, & Ford, 1988; Cramer & Brilliant, 2001; Cramer & Gaul, 1988; Hibbard et al., 1994; Hibbard & Porcerelli, 1998; Hibbard et al., 2000; Porcerelli, Thomas, Hibbard, & Cogan, 1998). Coefficients (alpha) of internal consistency for eight cards were .52 for denial, .71 for projection, and .77 for identification (Cramer, 1991b) and for six cards, .56 for denial, .69 for projection, and .58 for identification (Hibbard et al., 1994).
Validity
Four cross-sectional studies (Cramer 1987; Cramer & Brilliant, 2001; Cramer & Gaul, 1988; Porcerelli et al., 1998) and one cross-lagged longitudinal study (Cramer, 1997a) using the DMM have demonstrated predictable developmental changes in children’s use of defenses. The cognitively simpler defense of denial predominates during early years, the more cognitively complex defense of projection predominates during adolescence, and the most cognitively complex defense of identification predominates in adulthood. Cramer and Brilliant (2001) tested the hypothesis that once a child understands a particular defense, it no longer serves its purpose and is therefore given up and a more complex defense takes its place. As predicted, younger children (ages 7 through 8) who understood the defense of denial were less likely to use denial and older children (ages 9 through 11) who understood the defense of projection were less likely to use projection. In another longitudinal study, Cramer and Block (1998) predicted the use of denial in 23-year-old males from ratings of low ego resiliency and psychological difficulties at ages 3 through 4. Consistent with other features of denial as a gender syntonic defense, preschool assessments of girls did not predict use of denial at age 23. Cramer et al. (1988) reported significant relationships between higher levels of psychopathology and poorer interpersonal functioning and the use of lower level defenses of denial and projection. In addition, men with gender role conflict (i.e., a predominantly feminine personality organization) showed greater defense use than men with predominantly gender-consistent personality organization. An increase in defense use was also found in college students when given (bogus) gender-inconsistent feedback, thus threatening their sense of gender identity (Cramer, 1998b). Contrary to predictions, patients identified as having
472 Projective Assessment of Defense Mechanisms
anaclytic and introjective personality styles did not differ in the use of DMM defenses. Cramer and Blatt (1990) reported a decreased use of defenses in a sample of inpatients who underwent approximately 15 months of intensive psychoanalytic psychotherapy. A decrease in defense use was associated with a decrease in psychiatric symptoms. In a study of preadolescent boys who witnessed a traumatic death of a peer by lightning during a soccer game, Dollinger and Cramer (1990) found that boys who exhibited higher total defense scores were rated by clinicians as having less emotional upset than boys with lower defenses scores. Consistent with theory, defense use protected boys from excessive anxiety. In an experimental study (Cramer & Gaul, 1988), children exposed to a “failure” condition used more defenses (especially denial and projection) than children exposed to a “success” condition. The success group used more identification—the most mature defense. In another experimental study (Cramer, 1991a), college students exposed to a “criticism” condition used more defenses than prior to the condition and more than control subjects. Hibbard et al. (1994) reported that patients on an acute psychiatric ward used more denial and projection and less identification than a control group of college undergraduates. Psychiatric patients also exhibited a higher percentage of primitive defenses (i.e., the aggregate of primitive denial, projection, and identification divided by the total number of defenses) than the control group. A factor analysis lent support for the three clusters of DMM defenses. In a college student sample, Hibbard and Porcerelli (1998) provided additional support for a developmental hierarchy of defenses, for the three-factor structure of the DMM, and for distinguishing between mature and immature levels for denial and identification. The distributions of the scales were relatively normal except for immature identification and mature denial (both defenses comprise only two of seven levels of their parent scales). Greater relative use of identification in women in comparison to men replicated the earlier work of Cramer (1987). Support for convergent and discriminant validity of DMM mature and immature scores was reported through correlations with the mature and immature scores from a self-report measure of defense—the Defensive Style Questionnaire (Bond, Gardner, Christian, & Sigal, 1983). Using a prototype approach to assess borderline, psychopathic, narcissistic, and histrionic personality syndromes, Cramer (1999) reported significant relationships between the syndromes and the use of denial and projection. Immature denial was the strongest predictor of the borderline and histrionic syndrome while immature projection was the strongest predictor for the psychopathic and narcissistic syndrome. Porcerelli, Abramsky, Hibbard, and Kamoo (2001) reported a reliance on immature denial and immature projection in a case study of a serial sexual homicide perpetrator who met criteria for psychopathy.
Cross-Cultural Studies
Hibbard et al. (2000) assessed the differential validity of the DMM between an Asian American and White sample. Whites had higher mean scores for denial. No differences were found for projection, identification, or total defense scores. Surprisingly, DMM scales were slightly stronger predictors of desirable variables for Asian Americans and undesirable variables for Whites.
Strengths
The DMM is solidly grounded in psychoanalytic theories of defense and cognitive developmental theory. Interrater reliability of DMM scales has ranged from adequate to good, with consistently good total defense reliability coefficients. Support for internal consistency of the scales has also been provided by Cramer and others. Validation studies have been conducted both within and outside Cramer’s lab for the notion of a developmental hierarchy of defenses. Experimental studies have demonstrated predicted changes in defense scores following negative emotional conditions. Changes in defense use as a function of intensive psychotherapy have also been reported. Studies have demonstrated a relationship between the use of immature defenses (denial and projection), psychopathology, and poor interpersonal functioning. Convergent, discriminant, and construct validity have been reported for the mature/immature classification of DMM defenses and immature levels of denial and projection have been predictors of various personality syndromes. The DMM can be used with children, adolescents, and adults.
Limitations
Although the three DMM defenses represent different points along a developmental continuum, the use of only three defenses limits its clinical use. Therefore the DMM is only able to provide researchers and clinicians with an estimate of the level of defensive and personality functioning. Like the LDS and RDS, the DMM requires highly specific clinical training for interpretation.
SUMMARY AND CONCLUSIONS
This chapter provides a review of the three most prominent and clinically adaptable defense mechanisms assessment scales for projective test data: the Lerner Defense Scale, the Rorschach Defense Scales, and Defense Mechanism Manual. The authors of each of these scales provide detailed scoring criteria, allowing raters to obtain adequate to high levels of interrater reliability. Validity data is also provided for each scale. Although all three scales have demonstrated their usefulness as research instruments, these scales lack large standardization samples. However, the available validity studies do provide data from which to generate clinical hypotheses. As part of a comprehensive psychological test battery, these scales can provide useful information about healthy as well as pathological personality functioning, level of personality organization, regressive potential in psycho-dynamic therapies, treatment outcome, and psycho-dynamic case formulations.
In recent years, the field of psychology has placed the study of psychological health on equal footing with the study of psychopathology. This is exemplified in the work of Cramer (1995, 1997b, 1998a), who has been studying the relationship between the defense of identification and its relationship to identity formation in adolescents. Clinically, this “healthy” shift has underscored the need to assess healthy and adaptive aspects of personality functioning (Vaillant, 2000), especially in individuals with psychological disturbances. The RDS and the DMM provide a range from relatively mature/healthy defenses to relatively immature/pathological defenses. Although all three projective scales in this chapter include pathological defenses, the RDS appears best suited for this purpose because it contains both borderline- and psychotic-level defenses. The levels of defenses provided by the RDS—neurotic, borderline, and psychotic—are consistent with Kernberg’s (1975) psycho-structural categories, making the RDS a particularly useful instrument for the assessment of an individual’s predominant level of personality organization. However, both the LDS and RDS have been successful in differentiating borderline personality disorder from groups with greater and lesser severity. In addition, the immature denial and immature projection categories of the DMM show promise in the assessment of personality pathology.
The presence of borderline- or psychotic-level defenses can alert clinicians about the regressive potential of individuals who present for insight-oriented psychotherapy. These data can inform clinicians about necessary modifications (e.g., increased structure) to more traditional therapeutic strategies. All three defense scales provide for the assessment of pathological defenses.
Projective defense scales have proven useful in gauging the success of psycho-dynamic or insight-oriented psychotherapies. Clinicians can compare baseline assessments of defenses with assessments at certain points during psychotherapy or at termination. With the LDS, RDS, and DMM, comparisons in
presence or absence of defense and total defense use can be made. Total defense use has been shown to decrease as a function of psychotherapy. In cases of severe trauma, an increase of defense use can be a sign of improvement. With the RDS and DMM, relative defense scores for each of three levels can be obtained. Relative scores are calculated by dividing the number of defenses within each level by the total number of defenses. Relative scores provide a common metric for comparing defense use across different levels of defensive functioning. For example, at the end of a successful psychotherapy, a client’s relative defense scores may go from 15% psychotic level, 50% borderline level, and 35% neurotic level, to 0% psychotic level, 30% borderline defenses, and 70% neurotic defenses.
Lastly is the issue of defenses and dynamic case formulation. It is not enough for clinicians to assess the presence or absence of defenses. For purposes of psychotherapeutic technique, it is also important to determine whether a defense is used situationally—that is, in response to an immediate stressor—or is a more enduring, chronic, and sometimes what is referred to as character defense. This can be done through a combination of psychological testing and interview. Situational defenses can be immediately discussed by therapist and patient in order to aid the patient in developing a more adaptive approach to a stressor. Unlike situational defenses, more chronic and enduring defenses involve a slower and more complex process of making what is ego-syntonic more egodystonic (McWilliams, 1999).
REFERENCES
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
- Bond, M., Gardner, S.T., Christian, J., & Sigal, J.J. (1983). Empirical study of self-rated defense styles. Archives of General Psychiatry, 40, 333–338.
- Bond, M., Paris, J., & Zweig-Frank, H. (1994). Defense style and borderline personality disorder. Journal of Personality Disorders, 8, 28–31.
- Brenner, C. (1955). An elementary textbook of psychoanalysis. New York: International Universities Press.
- Brenner, C. (1982). Mind in conflict. New York: International Universities Press.
- Cooper, S.H., Perry, J.C., & Arnow, D. (1988). An empirical approach to the study of defense mechanisms: 1. Reliability and preliminary validity of the Rorschach Defense Scales. Journal of Personality Assessment, 52, 187–203.
474 Projective Assessment of Defense Mechanisms
- Cooper, S.H., Perry, J.C., & O’Connell, M.E. (1991). The Rorschach Defense Scales: 2. Longitudinal perspectives. Journal of Personality Assessment, 56, 191–201.
- Cramer, P. (1987). The development of defense mechanisms. Journal of Personality, 55, 597–614.
- Cramer, P. (1991a). Anger and the use of defense mechanisms in college students. Journal of Personality, 59, 39–55.
- Cramer, P. (1991b). The development of defense mechanisms: Theory, research, and assessment. New York: Springer-Verlag.
- Cramer, P. (1995). Identity, narcissism, and defense mechanisms in late adolescence. Journal of Research in Personality, 29, 341– 361.
- Cramer, P. (1997a). Evidence for change in children’s use of defense mechanisms. Journal of Personality, 65, 233–247.
- Cramer, P. (1997b). Identity, personality and defense mechanisms: An observer based study. Journal of Research in Personality, 31, 58–77.
- Cramer, P. (1998a). Freshmen to senior year: A follow-up study of identity, narcissism and defense mechanisms. Journal of Research in Personality, 32, 156–172.
- Cramer, P. (1998b). Threat to gender representation: Identity and identification. Journal of Personality, 66, 335–357.
- Cramer, P. (1999). Personality, personality disorders, and defense mechanisms. Journal of Personality, 67, 535–554.
- Cramer, P., & Blatt, S.J. (1990). Use of the TAT to measure change in defense mechanisms following intensive psychotherapy. Journal of Personality Assessment, 54, 236–251.
- Cramer, P., Blatt, S.J., & Ford, R.Q. (1988). Defense mechanisms in the anaclitic and introjective personality configuration. Journal of Consulting and Clinical Psychology, 56, 610–616.
- Cramer, P., & Block, J. (1998). Preschool antecedents of defense mechanism use in young adults: A longitudinal study. Journal of Personality and Social Psychology, 74, 159–169.
- Cramer, P., & Brilliant, M.A. (2001). Defense use and defense understanding in children. Journal of Personality, 69, 297–322.
- Cramer, P., & Davison, K. (Eds.) (1998). Defense mechanisms in contemporary personality research [Special issue]. Journal of Personality, 66, 879–1157.
- Cramer, P., & Gaul, R. (1988). The effects of success and failure on children’s use of defense mechanisms. Journal of Personality, 56, 729–742.
- Devens, M., & Erickson, M.T. (1998). The relationship between defense styles and personality disorders. Journal of Personality Disorders, 12, 86–93.
- Dollinger, S.J., & Cramer, P. (1990). Children’s defensive responses and emotional upset following a disaster: A projective assessment. Journal of Personality Assessment, 54, 116–127.
- Freud, A. (1936). The ego and the mechanisms of defense. New York: International Universities Press.
- Freud, S. (1894). The neuro-psychoses of defense (Standard ed., Vol. 3, pp. 43–68).
- Freud, S. (1896). Further remarks on the neuro-psychoses of defense (Standard ed., Vol. 3, pp. 159–185).
- Freud, S. (1923). The ego and the id (Standard ed., Vol. 19, pp. 3–66).
- Freud, S. (1926). Inhibitions, symptoms, and anxiety (Standard ed., Vol. 20, pp. 77–175).
- Gacono, C.B. (1990). An empirical study of object relations and defensive operations in antisocial personality. Journal of Personality Assessment, 54, 589–600.
- Gacono, C.B., Meloy, J.R., & Berg, J.L. (1992). Object relations, defensive operations, and affective states in narcissistic, borderline, and antisocial personality disorder. Journal of Personality Assessment, 59, 32–49.
- Hare, R. (1985). Comparison of procedures for the assessment of psychopathy. Journal of Consulting and Clinical Psychology, 53, 7–16.
- Hibbard, S., Farmer, L., Wells, C., Difillipo, E., Barry, W., Korman, R., et al. (1994). Validation of Cramer’s Defense Mechanism Manual. Journal of Personality Assessment, 63, 197–210.
- Hibbard, S., & Porcerelli, J. (1998). Further validation of Cramer’s Defense Mechanism Manual. Journal of Personality Assessment, 70, 460–483.
- Hibbard, S., Tang, P.C.Y., Latko, R., Park, J.H., Munn, S., Bolz, B., et al. (2000). Differential validity of the Defense Mechanism Manual for the TAT between Asian Americans and Whites. Journal of Personality Assessment, 75, 351–372.
- Hilsenroth, M.J., Hibbard, S., Nash, M.R., & Handler, L. (1993). A Rorschach study of narcissism, defense and aggression in borderline, narcissistic, and cluster personality disorders. Journal of Personality Assessment, 60, 346–361.
- Holt, R. (1970). Manual for scoring primary process on the Rorschach. Unpublished manuscript.
- Holt, R. (1977). A method for assessing primary process manifestations and their control in Rorschach responses. In M. Rickers-Ovsiankina (Ed.), Rorschach psychology (pp. 375–420). New York: Krieger.
- Kernberg, O. (1967). Borderline personality organization. Journal of the American Psychoanalytic Association, 15, 641–685.
- Kernberg, O. (1975). Borderline conditions and pathological narcissism. New York: Jason Aronson.
- Kernberg, O. (1976). Object relations theory and clinical psychoanalysis. New York: Jason Aronson.
- Kernberg, O. (1984). Severe personality disorders: Psychotherapeutic strategies. New Haven, CT: Yale University Press.
- Klein, M. (1946). Some notes on the schizoid mechanisms. International Journal of Psychoanalysis, 27, 99–110.
- Kohut, H. (1977). The restoration of the self. New York: International Universities Press.
- Kohut, H. (1984). How does analysis cure? Chicago: University of Chicago Press.
- Lerner, H., Albert, C., & Walsh, M. (1987). The Rorschach assessment of borderline defense: A concurrent validity study. Journal of Personality Assessment, 51, 334–348.
- Lerner, H., Sugarman, A., & Gaughran, J. (1981). Borderline and schizophrenic patients: A comparative study of defensive structure. Journal of Nervous and Mental Disease, 169, 705–711.
- Lerner, P. (1990). Rorschach assessment of primitive defense: A review. Journal of Personality Assessment, 54, 30–46.
- Lerner, P., & Lerner, H. (1980). Rorschach assessment of primitive defenses in borderline personality structure. In J. Kwawer, H. Lerner, P. Lerner, & A. Sugarman (Eds.), Borderline phenomena and the Rorschach test (pp. 257–274). Madison, CT: International Universities Press.
- Lerner, P., & Van-Der Keshet, Y. (1995). A note on the assessment of idealization. Journal of Personality Assessment, 65, 77–90.
- Mayman, M. (1967). Object representations and object relationships in Rorschach responses. Journal of Projective Techniques and Personality Assessment, 31, 17–24.
- McWilliams, N. (1999). Psychoanalytic case formulation. New York: Guilford Press.
- Modell, A. (1975). A narcissistic defense against affects and the illusion of self-sufficiency. International Journal of Psychoanalysis, 56, 275–282.
- Murray, H.A. (1943). The Thematic Apperception Test. Cambridge, MA: Harvard University Press.
- Perry, J.C. (1993). Defenses and their affects. In N.E. Miller, L. Luborsky, J.P. Barber, and J.P. Docherty (Eds), Psychoanalytic treatment research: A handbook for clinical practice (pp. 274– 306). New York: Basic Books.
- Perry, J.C., Hoglend, P., Shear, K., Vaillant, G.E., Horowitz, M.J., Kardos, M.E., et al. (1998). Field trial of a diagnostic axis for DSM-IV. Journal of Personality Disorders, 12, 1–13.
- Pinheiro, R.T., Sousa, P.R., Da Silva, R.A., Horta, B.L., De Souza, R.M., & Fleming, M. (2001). Cocaine addicts and their families: An empirical study of the processes of identification. International Journal of Psychoanalysis, 82, 347–360.
- Porcerelli, J.H., Abramsky, M.F., Hibbard, S., & Kamoo, R. (2001). Object relations and defense mechanisms of a psychopathic serial sexual homicide perpetrator: A TAT analysis. Journal of Personality Assessment, 77, 87–104.
- Porcerelli, J.H., Thomas, S., Hibbard, S., & Cogan, R. (1998). Defense mechanisms development in children, adolescents, and late adolescents. Journal of Personality Assessment, 71, 411–420.
- Pruitt, W., & Spilka, B. (1964). Rorschach Empathy-Object Relationship Scale. In P. Lerner (Ed.). Handbook of Rorschach scales (pp. 315–323). New York: International Universities Press.
- Rorschach, H. (1942). Psychodiagnostics. New York: Grune & Stratton.
- Schafer, R. (1954). Psychoanalytic interpretation of Rorschach testing. New York: Grune & Stratton.
- Schafer, R. (1968). Mechanisms of defense. International Journal of Psychoanalysis, 49, 49–62.
- Stolorow, R., and Lachman, R. (1980). The psychoanalysis of developmental arrest. New York: International Universities Press.
- Sugarman, A. (1980). The borderline personality organization as manifested on psychological tests. In J. Kwawer, H. Lerner, P. Lerner, & A. Sugarman (Eds.), Borderline phenomena and the Rorschach test (pp. 39–57). Madison, CT: International Universities Press.
- Vaillant, G.E. (1971). Theoretical hierarchy of adaptive ego mechanisms. Archives of General Psychiatry, 24, 107–118.
- Vaillant, G.E. (1976). Natural history of male psychological health: V. Archives of General Psychiatry, 33, 535–545.
- Vaillant, G.E. (1977). Adaptation to life. Boston: Little, Brown.
- Vaillant, G.E. (1992). Ego mechanisms of defense: A guide for clinicians and researchers. Washington, DC: American Psychiatric Press.
- Vaillant, G.E. (1993). The wisdom of the ego. Cambridge, MA: Harvard University Press.
- Vaillant, G.E. (2000). Adaptive mental mechanisms: The role of positive psychology. American Psychologist, 55, 89–98.
- Weiner, I.B. (1966). Psychodiagnosis in schizophrenia. New York: Wiley.
- Willick, M.S. (1995). Defense. In B.E. Moore & B.D. Fine (Eds.), Psychoanalysis: The major concepts (pp. 485–493). New Haven, CT: Yale University Press.
- Winnicott, D. (1953). Transitional objects and transitional phenomena. International Journal of Psychoanalysis, 34, 89–97.
- Winnicott, D. (1965). Ego distortion in terms of true and false self. In D. Winnicott (Ed.), The maturational process and the facilitating environment (pp. 140–152). Madison, CT: International Universities Press.
Projective Assessment of Interpersonal Dependency
ROBERT F. BORNSTEIN
DEFINING DEPENDENCY 476
THE EVOLUTION OF DEPENDENCY: FROM PSYCHO-
DYNAMIC CONCEPT TO PSYCHOMETRIC CONSTRUCT
477
PROJECTIVE ASSESSMENT OF INTERPERSONAL
DEPENDENCY: VARIETY, VALIDITY, STRENGTH, AND
LIMITATION 477 Widely Used Projective Dependency Measures 477 Criterion Validity of Projective Dependency Tests 479 Criterion Validity in Context: Comparison With Self-Report Data 479
Strengths and Limitations of Projective Dependency Tests 480
If a professional psychologist is evaluating you in a situation in which you are at risk and asks you for responses to ink blots . . . walk out of that psychologist’s office. Going through with such an examination creates the danger of having a serious decision made about you on totally invalid grounds.
—Dawes (1994, pp. 152–153)
Dawes’s (1994) harsh assessment is blunter than most, but it has been echoed by numerous critics who question the validity of projective assessment techniques in general (Hunsley & Bailey, 1999; Lilienfeld, Wood, & Garb, 2000), and projective tests of dependency in particular (Wood, Lilienfeld, Garb, & Nezworski, 2000). Not all psychologists are skeptical regarding the utility of projective assessment tools, however. Responding to the criticisms of Dawes (1994) and others, some researchers have argued that projective measures of interpersonal dependency are both clinically useful and psychometrically sound (Viglione, 1999; Weiner, 2000).
Who is correct—the skeptics or the supporters? As is so often the case in scientific psychology, both are, but in different ways.
This chapter reviews research on the projective assessment of interpersonal dependency, to delineate the strengths and limitations of projective dependency tests and determine which THE FUTURE OF PROJECTIVE DEPENDENCY ASSESSMENT: FROM PARTICIPANT CLASSIFICATION TO PROCESS DISSOCIATION 480 The Inter- and Intrapersonal Dynamics of Dependency Assessment 480 Exploring Objective/Projective Test Score Discontinuities 480 Clinical and Research Implications 481 CONCLUSION 481 NOTES 482 REFERENCES 482
instruments—if any—are useful in research and clinical settings. I begin by presenting a broad definition of interpersonal dependency, to place the ensuing discussion in context. I then trace the evolution of the dependency construct in psychology and the implications of this evolution for our understanding of dependent personality traits. Next, I evaluate widely used projective instruments for assessing interpersonal dependency, both individually and collectively, and contrast these instruments with self-report dependency measures. Finally, I outline a conceptual framework for integrating projective and self-report test data and assess current trends and future directions in projective dependency testing.
DEFINING DEPENDENCY
There have been more than 600 published studies examining the etiology and dynamics of dependent personality traits (Bornstein, 1993, 1996a). Research in this area has been facilitated by the emergence of a consensus regarding the core traits that comprise a dependent personality orientation (Birtchnell, 1988; Millon, 1996; Pincus & Gurtman, 1995). As Bornstein (1992, 1993) noted, any comprehensive definition of interpersonal dependency must include four components: (1) motivational (i.e., a marked need for guidance, support, and approval from others); (2) cognitive (i.e., a perception of oneself as powerless and ineffectual, coupled with the belief that others are comparatively powerful and potent); (3) affective (i.e., a tendency to become anxious and fearful when required to function autonomously); and (4) behavioral (i.e., a tendency to seek support and reassurance from others and engage in self-presentation strategies designed to strengthen relationships with potential caregivers).
As Pincus and Gurtman (1995) noted, this broad, fourcomponent definition not only captures the core features of interpersonal dependency but is also consistent with empirical findings regarding situational variability in dependencyrelated behavior and emotional responding (e.g., Bornstein, Bowers, & Bonner, 1996a), and with studies delineating the adaptive features of dependent personality traits (e.g., Bornstein, Riggs, Hill, & Calabrese, 1996).
THE EVOLUTION OF DEPENDENCY: FROM PSYCHO-DYNAMIC CONCEPT TO PSYCHOMETRIC CONSTRUCT
Research on interpersonal dependency began in earnest with Freud’s (1905) seminal work examining the role of oral fixation in the etiology and dynamics of dependent personality traits. Freud hypothesized that frustration or overgratification during the infantile “oral” stage would lead to an oral dependent personality style characterized by: (1) continued dependence on other people for nurturance, guidance, protection, and support; and (2) reliance on food- and mouthrelated activities (e.g., smoking, eating) as a means of managing anxiety.
Although research does not support either of Freud’s original (1905) hypotheses, Freud’s work in this area was heuristic, stimulating numerous empirical investigations and alternative theoretical viewpoints (Bornstein, 1996a). In fact, many early factor analytic studies analyzing components of the dependent personality tested Freudian models of oral dependency (e.g., Goldman-Eisler, 1950; Lazare, Klerman, & Armor, 1966). Social learning frameworks that dominated dependency research in the 1960s arose, in part, as a reaction to earlier psycho-dynamic views on this topic, shifting the emphasis from infantile experience to gender role socialization as a key factor in the etiology of dependency (Sears, Rau, & Alpert, 1965; Walters & Parke, 1964). With the development of cognitive models of dependency in the early 1990s (Bornstein, 1992, 1993), research in this area drifted still further from its psychoanalytic roots, although vestiges of earlier dynamic hypotheses continue to emerge in theoretical refinements and empirical studies (Bornstein, 1996a).
Different theoretical perspectives on dependency differ in numerous ways, but they all assume that dependent personality traits can be usefully categorized into subtypes, with each subtype having contrasting surface features and underlying dynamics. Initial work in this area attempted to distinguish “oral optimists” from “oral pessimists” based on inferred developmental antecedents and current psychopathology (Goldman-Eisler, 1950). Later social learning frameworks devoted considerable attention to distinguishing instrumental from emotional dependency and assessing the covariation between the two (Baltes, 1996; Heathers, 1955). Most recently, researchers distinguished self-attributed (i.e., openly acknowledged) from implicit (i.e., unconscious, unacknowledged) dependency strivings (Bornstein, 1998a, 1998b). This latter distinction has had a strong impact on research involving projective dependency tests.
PROJECTIVE ASSESSMENT OF INTERPERSONAL DEPENDENCY: VARIETY, VALIDITY, STRENGTH, AND LIMITATION
To date, more than 40 separate instruments for assessing interpersonal dependency have been developed. The majority of these instruments are self-report measures, followed by projective tests and structured interviews. Although self-report and projective tests are used in a wide range of research and clinical settings, most interview measures are specifically designed to assess dependent personality disorder (DPD) symptoms and are found primarily in treatment settings. Behavioral (i.e., observational) measures of dependency are used almost exclusively with nursery school, kindergarten, or elementary school children, in classroom settings or the home (Bornstein, 1993).
Widely Used Projective Dependency Measures
Considerable effort has gone into assessing individual differences in implicit dependency strivings, and projective tests of dependency have been widely available since the late 1940s. Although at least a dozen separate projective dependency measures have been used at one time or another, five projective dependency tests account for the vast majority of published studies on this topic.1 In the following sections, I describe the essential features of these five measures.
Rorschach Oral Dependency (ROD) Scale
Masling, Rabie, and Blondheim’s (1967) ROD scale has been by far the most widely used projective measure of dependency during the past 30 years, accounting for more than 80% of published research in this area (Bornstein, 1996b, 1999). Masling et al.’s scoring system was derived from Schafer’s (1954) speculations regarding psychoanalytic content in Rorschach responses. As a result, it has strong classical psychoanalytic roots.
Because standard ROD scoring involves only the freeassociation portion of a participant’s Rorschach responses, ROD scores can be derived from individually administered Rorschach protocols or from free associations collected in a group setting (Masling, 1986). In either case, the participant receives one point for any Rorschach response that falls into any of the following categories: (1) foods and drinks; (2) food sources; (3) food objects; (4) food providers; (5) passive food receivers; (6) begging and praying; (7) food organs; (8) oral instruments; (9) nurturers; (10) gifts and gift givers; (11) good luck symbols; (12) oral activity; (13) passivity and helplessness; (14) pregnancy and reproductive anatomy; (15) “baby talk” responses (e.g., “bunny rabbit,” “kitty cat”); and (16) negations of oral percepts (e.g., “man with no mouth”). In the group administration of the ROD scale, each participant provides 25 written responses; three each to Cards I, II, III, VIII, and X, and two responses to each of the remaining cards (Masling, 1986). To control for variations in response productivity in individually administered Rorschach protocols, ROD scores are expressed as percentages (i.e., the number of oral dependent Rorschach responses divided by R).
ROD scores show excellent interrater reliability and adequate retest reliability over 16-, 28-, and 60-week intertest intervals (Bornstein, Rossner, & Hill, 1994). The convergent validity of the test is well established: ROD scores predict help-seeking, conformity, compliance, suggestibility, and interpersonal yielding in laboratory and field settings (Bornstein, 1996b), and show the expected relationships with questionnaireand interview-derived Axis II diagnoses (Bornstein, 1998b; Bornstein, Hilsenroth, Padawer, & Fowler, 2000). The discriminant validity of ROD scores is supported by findings showing that these scores are only minimally related to social desirability, IQ, and locus of control (Bornstein & O’Neill, 1997). Clinical and college student norms for the ROD scale are provided by Bornstein et al. (2000) and Bornstein, Bonner, Kildow, and McCall (1997).
Thematic Apperception Test (TAT) Dependency Scale
Originally developed by Kagan and Mussen (1956), the TAT dependency scale is based on Murray’s (1938) description of need for succorance (n Succorance) and its manifestation in TAT responses. TAT dependency scale scoring is somewhat less standardized than that of the ROD scale, and some investigators have incorporated into the scoring system content from other of Murray’s need dimensions (e.g., need for affiliation; see Masling et al., 1967; Zuckerman & Grosz, 1958). Like ROD scores, TAT dependency scores can be derived from individually administered protocols or from protocols collected in a group setting.
Psychometric data for the TAT dependency scale are spotty, and the retest reliability and discriminant validity of the scale have never been assessed. These limitations—coupled with the absence of clinical norms—make its use in treatment settings problematic. However, TAT-based dependency assessment has seen a resurgence during the past decade, following publication of McClelland, Koestner, and Weinberger’s (1989) review of TAT measures of implicit need states. If current trends persist, it is likely that gaps in the psychometric literature on the TAT dependency scale will be filled during the coming years.
Blacky Test Oral Dependency Scale (BTODS)
The BTODS is based on Blum’s (1949) system for deriving oral dependent content from responses to the Blacky Pictures, a set of 12 cartoons depicting four members of a canine family (the genderless main character Blacky, sibling Tippy, Mama, and Papa). In different cards, characters interact in psycho-dynamically loaded situations (e.g., Blacky breastfeeding, defecating, having an erotic dream about his mother, having his tail chopped off). Only those cards with oral content are used to calculate BTODS scores.
The convergent validity of the BTODS is quite good (Bornstein, 1999), although few studies have assessed the discriminant validity of BTODS scores (cf., Weiss, 1969). Interrater and retest reliability data support the utility of the scale (Lanyon & Goodstein, 1997), although some researchers have suggested that while these reliability data are strong enough to draw general group inferences in research studies, they are not strong enough to permit precise assessment of individual patients in clinical settings (Sappenfield, 1965). Research and clinical use of the BTODS has declined precipitously in recent years.
Holtzman Inkblot Test (HIT) Dependency Scale
S. Fisher’s (1970) HIT dependency scale is analogous in certain respects to Masling et al.’s (1967) ROD scale. Like the ROD scale, the HIT dependency scale is derived from participants’ free associations to a standard set of inkblots. However, because HIT dependency scores are derived from participants’ associations to the Holtzman (1961) inkblots, they have a potential advantage over ROD scale scores: The
| ROD |
21 |
1,320 |
.37 |
8.49 |
#.001 |
538 |
| BTODS |
6 |
323 |
.50 |
4.51 |
#.001 |
39 |
| TAT |
4 |
125 |
.34 |
2.84 |
#.001 |
8 |
| HIT |
1 |
40 |
.12 |
0.31 |
NS |
— |
TABLE 35.1 Criterion Validity Coefficients for Projective Dependency Tests
Note. Originally published as Table 2 in “Criterion Validity of Objective and Projective Dependency Tests: A Meta-Analytic Assessment of Behavioral Prediction,” by R.F. Bornstein, 1999, Psychological Assessment, 11, 48–57. Copyright % 1999 by the American Psychological Association. Reprinted with permission.
two parallel forms of the Holtzman inkblots allow researchers to assess short-term retest reliability (Hill, 1972) and the effects of various experimental manipulations using a pre-/ postdesign (J.M. Fisher & S. Fisher, 1975).
Despite its advantages, there have been few published investigations involving the HIT dependency scale (Bornstein, 1993, 1999). Those that do exist report good interrater reliability and convergent validity (Leichsenring, 1991). No longterm retest reliability data are available for the scale, nor have clinical or nonclinical norms been published. Clinical and research interest in the scale has waned since the 1970s.
Early Memories Dependency Probe (EMDP)
Fowler, Hilsenroth, and Handler’s (1996) EMDP represents a promising new tool for the projective assessment of dependency. Based in part on Mayman’s (1968) procedures for assessing the qualities of an individual’s internalized object representations through an early memory interview, EMDP scoring involves assigning a single 7-point rating that captures the overall tone of an individual’s earliest eating-related memory (1 ” clear conflict over dependency needs; 4 ” healthy, positive associations; 7 ” strongly negative associations). EMDP scores can be derived from newly administered early memory interviews or from archival interview data (Fowler et al., 1996; Fowler, Hilsenroth, & Handler, 2000).
Preliminary evidence supports the convergent and discriminant validity of the EMDP scale (Fowler et al., 1996, 2000). Although interrater reliability data are strong for various early memory rating dimensions (Karliner, Westrich, Shedler, & Mayman, 1996), the retest reliability of the EMDP has not been assessed, nor are clinical norms yet available.
Criterion Validity of Projective Dependency Tests
Although most test validation studies examine the relationship of test scores to questionnaire- and interview-derived data, this mode of construct validity assessment is problematic in many ways (Meyer, 1996; Meyer & Handler, 1997).
To assess the validity and utility of extant dependency tests, Bornstein (1999) conducted a meta-analysis of published studies using a strict inclusion criterion: Only those studies that validated objective or projective test scores against an observable dependency-related behavior (e.g., suggestibility, social help-seeking, medical help-seeking) were included in the sample. The literature search revealed that the criterion validity of four projective dependency tests had been assessed against observable indices of dependent behavior (no published studies assessing behavioral correlates of EMDP scores were available at the time). Criterion validity data for these four measures are summarized in Table 35.1.
As Table 35.1 shows, every projective dependency test produced scores that were positively correlated with indices of overt dependent behavior. ROD scores (Masling et al., 1967) and TAT dependency scores (Kagan & Mussen, 1956) showed moderate positive correlations (according to Cohen’s [1977] criteria), while BTODS scores (Blum, 1949) showed a large positive correlation with indices of dependent behavior. HIT dependency scores (S. Fisher, 1970) were more modestly correlated with dependent behavior, and the HIT score-behavior correlation was nonsignificant.
In addition to assessing the criterion validity of individual dependency tests, Bornstein’s (1999) meta-analysis yielded an overall projective test score–dependent behavior effect size (calculated via a sample size weighted average of individual effect sizes). The 32 test score-behavior comparisons in Table 35.1 produced an overall criterion validity coefficient (r) of .37, with a combined z of 9.09 (p # .001).
Criterion Validity in Context: Comparison With Self-Report Data
Although a validity coefficient of .37 may seem modest, it is in line with those obtained for well-designed psychological assessment tools when behavioral criteria are used to evaluate test score validity (Baldwin & Sinclair, 1996). In fact, psychometrically sound questionnaire and interview trait measures typically report behaviorally referenced criterion validity coefficients in the .30 range (Mischel & Shoda, 1995).
In this context, it is worthwhile to contrast the criterion validity coefficient for projective dependency tests with that of self-report dependency measures. Criterion validity effect sizes (rs) for self-report tests in Bornstein’s (1999) metaanalysis ranged from .04 (for Blatt, D’Afflitti, & Quinlan’s [1976] Depressive Experiences Questionnaire dependency scale) to .46 (for Beck, Epstein, Harrison, & Emery’s [1983] Sociotropy-Autonomy Scale). The overall objective test score–dependent behavior effect size was .31, with a combined z of 8.67 (p # .001).
A focused comparison of effect sizes indicated that the validity coefficients for projective and self-report dependency tests did not differ (Z ” 1.21, NS). Thus, Bornstein’s (1999) meta-analytic results indicate that, in general, projective and objective dependency tests have comparable criterion validity.2
Strengths and Limitations of Projective Dependency Tests
Projective and self-report dependency tests have comparable criterion validity, but each type of test has its own strengths and limitations. Among the most important advantages of projective dependency tests are their resistance to self-report and self-presentation effects (Bornstein, Bowers, & Bonner, 1996b) and to outright faking on the part of participants (Bornstein, Rossner, Hill, & Stepanian, 1994). In addition, the low face validity of projective dependency tests minimizes gender role confounds that may artificially decrease men’s reports of dependent traits and experiences when questionnaire measures are used (Bornstein, 1995). Although no studies have assessed the effects of cultural background on projective dependency test scores, the same qualities that minimize self-report and self-presentation effects in other contexts should also minimize the impact of cultural background on projective dependency scores. (In contrast, studies have demonstrated repeatedly that individuals from sociocentric cultures obtain significantly higher self-report dependency scores than do individuals from more individualistic cultures; see Bornstein, 1992, 1993.)
Of course, projective dependency tests have some limitations as well. Among the most important limitations of projective dependency tests relative to questionnaires are: (1) their relative inefficiency (they are time consuming and labor intensive, especially when administered individually); (2) their susceptibility to subtle mood effects (Bornstein, Bowers, & Bonner, 1996a); and (3) their covariation with stress and psychopathology levels (J.M. Fisher & S. Fisher, 1975).
THE FUTURE OF PROJECTIVE DEPENDENCY ASSESSMENT: FROM PARTICIPANT CLASSIFICATION TO PROCESS DISSOCIATION
A paradox has emerged in the dependency assessment literature: Even though self-report and projective dependency measures both predict theoretically related features of behavior (e.g., help-seeking), scores on the two tests correlate modestly with each other. When Bornstein (2002) integrated findings from 12 published studies examining objectiveprojective dependency test score relationships, he found a mean intertest intercorrelation (r) of .29. How is it possible that two modes of dependency assessment both predict dependent behavior, while the score on one type of test only accounts for a small portion of the variance in the other test score? Exploration of this paradox provides a wealth of information regarding the future of projective dependency assessment and optimal use of self-report and projective dependency tests in research and clinical settings.
The Inter- and Intrapersonal Dynamics of Dependency Assessment
Beginning with the work of Masling (1960), Rosenthal (1966), and others (e.g., Sattler & Winget, 1970), clinicians and educators have recognized the need to interpret assessment results within the context of the interpersonal milieu in which test data were obtained. In this context, the face validity of an assessment tool may be an important moderating variable in test score-behavior relationships. Studies show that face validity can influence participants’ emotional reactions and test responses on a wide variety of measures (Nevo, 1985; Nevo & Svez, 1985). Clearly, part of the reason that objective and projective dependency tests are only modestly intercorrelated is that some participants deliberately choose to underor overreport dependent traits and behaviors on self-report tests (which have high face validity), but cannot deliberately alter their scores on projective dependency tests with low face validity (Bornstein, Rossner, Hill, & Stepanian, 1994). Objective and projective dependency tests are characterized by very different inter- and intrapersonal dynamics, and optimal use of both types of tests requires that clinicians and researchers consider these dynamics when interpreting test scores.
Exploring Objective/Projective Test Score Discontinuities
The modest intercorrelations of objective and projective dependency scores need not be seen as a problem. On the contrary, these modest test score intercorrelations provide an
Score on Objective Dependency Test
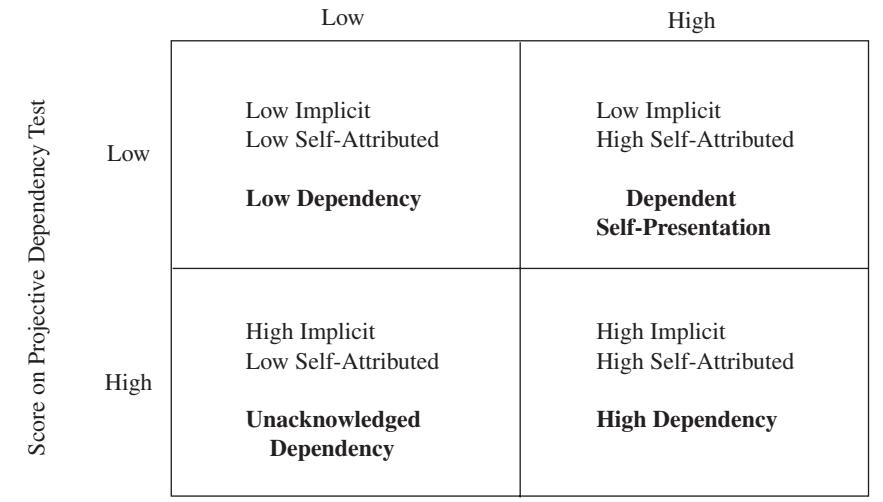
Figure 35.1 Continuities and discontinuities between implicit and self-attributed need states: A four-cell model. Originally published as Figure 1 in “Implicit and Self-Attributed Dependency Strivings,” by R.F. Bornstein, Journal of Personality and Social Psychology, 75, 778–787. Copyright % 1998 by the American Psychological Association. Reprinted with permission.
opportunity to examine naturally occurring discontinuities between implicit and self-attributed dependency needs.
Figure 35.1 illustrates four outcomes that can be obtained when objective and projective dependency tests are administered to the same person. As shown in the upper left and lower right quadrants of Figure 35.1, it is possible that a person will score high or low on both measures, which would indicate convergence between this person’s self-attributed and implicit dependency scores. The other two cells in Figure 35.1 illustrate discontinuities between implicit and explicit dependency needs. In one case (i.e., high projective dependency score coupled with low objective dependency score), a person has high levels of implicit dependency needs but does not acknowledge them. These individuals may be described as having unacknowledged dependency strivings. In the other case (i.e., low projective dependency score coupled with high objective dependency score), the person has low levels of implicit dependency needs but presents him- or herself as being highly dependent. These individuals may be described as having a dependent self-presentation.
Clinical and Research Implications
By administering objective and projective measures of a particular motive or need state to the same individual, clinicians and researchers can obtain a more complete picture of that person’s underlying and expressed strivings. Exploration of discontinuities can reveal important information regarding personality structure and interpersonal style (see Bornstein, 1998b, for preliminary results in this area). This type of discontinuity analysis can enhance the validity of dependency test data, because objective and projective dependency scores combined lead to more precise and accurate predictions than either type of test data alone.
Archer and Krishnamurthy (1993a, 1993b) applied the concept of incremental validity to objective-projective test score interrelationships, and consistent with this perspective, Bornstein (1998b) found that combining implicit and selfattributed dependency test scores increased the overall accuracy of behavioral prediction by capturing both “spontaneous” and goal-directed dependent behavior in different contexts and settings. Bornstein (1998a) found that individuals who reported high levels of DPD symptoms and those who reported high levels of histrionic personality disorder (HPD) symptoms both obtained elevated scores on the ROD scale (a measure of implicit dependency needs), whereas only DPD individuals obtained elevated scores on Hirschfeld et al.’s (1977) Interpersonal Dependency Inventory (a measure of self-attributed dependency needs). Thus, the two measures used together yielded richer diagnostic information than either test alone.
CONCLUSION
Dawes’s (1994, p. 153) assertion that agreeing to be evaluated by a projective test “creates the danger of having a serious decision made about you on totally invalid grounds” is technically correct, but misleading. True, some psychologists misuse projective test data, but the same is true of self-report data. Recent studies and meta-analyses indicate that projective tests are at least as valid as objective tests when used to assess individual differences in interpersonal dependency. When these results are coupled with findings showing that the scoring of many objective tests is far less “objective” than once thought (Allard, Butler, Faust, & Shea, 1995), we can qualify and reframe Dawes’s assertion: Agreeing to any sort of psychological evaluation creates some danger of having a “serious decision made about you on invalid grounds,” but there is no evidence that this occurs more frequently for projective than objective tests.
While research indicates that at least three widely used projective dependency tests have adequate criterion validity, only the ROD scale has an extensive enough research base to allow for assessment of individual patients in clinical and forensic settings (e.g., detailed norms, long-term retest reliability data). As time goes on, and additional findings accumulate, the EMDP might also emerge as a clinically useful assessment tool, but for this (and other) projective dependency tests, more extensive criterion validity data are needed, along with more detailed clinical and nonclinical norms.
NOTES
Other, less frequently used projective measures of dependency include sentence completion tests (Sinha, 1968), the Hand Test (Wagner, 1983), and Spontaneous Oral Associations (O’Neill, Greenberg, & Fisher, 1984).
It is informative to contrast these data with those reported for clinical interviews designed to assess DPD symptoms. Although there is ample evidence supporting the criterion validity of widely used projective and objective dependency tests, no published studies have assessed the criterion validity of DPD interview scores. Research in this area has been limited to assessing the reliability of DPD symptoms and the covariation of DPD symptom scores with scores on other questionnaire and interview measures. Not surprisingly, the DSM-IV DPD symptom criteria are not in line with current published research on the dynamics of interpersonal dependency (Bornstein, 1997).
REFERENCES
- Allard, G., Butler, J., Faust, D., & Shea, M.T. (1995). Errors in hand scoring objective personality tests. Professional Psychology, 26, 304–308.
- Archer, R.P., & Krishnamurthy, R. (1993a). Combining the Rorschach and MMPI in the assessment of adolescents. Journal of Personality Assessment, 60, 132–140.
- Archer, R.P., & Krishnamurthy, R. (1993b). A review of MMPI and Rorschach interrelationships in adult samples. Journal of Personality Assessment, 61, 277–293.
- Baldwin, M.W., & Sinclair, L. (1996). Self-esteem and “if . . . then” contingencies of interpersonal acceptance. Journal of Personality and Social Psychology, 71, 1130–1141.
- Baltes, M.M. (1996). The many faces of dependency in old age. Cambridge, England: Cambridge University Press.
- Beck, A.T., Epstein, N., Harrison, R.P., & Emery, G. (1983). Development of the Sociotropy-Autonomy Scale: A measure of personality factors in psychopathology. Unpublished manuscript, University of Pennsylvania School of Medicine, Philadelphia.
- Birtchnell, J. (1988). Defining dependence. British Journal of Medical Psychology, 61, 111–123.
- Blatt, S.J., D’Afflitti, J.P., & Quinlan, D.M. (1976). Experiences of depression in normal young adults. Journal of Abnormal Psychology, 85, 383–389.
- Blum, G.S. (1949). A study of the psychoanalytic theory of psychosexual development. Genetic Psychology Monographs, 39, 3–99.
- Bornstein, R.F. (1992). The dependent personality: Developmental, social, and clinical perspectives. Psychological Bulletin, 112, 3–23.
- Bornstein, R.F. (1993). The dependent personality. New York: Guilford Press.
- Bornstein, R.F. (1995). Sex differences in objective and projective dependency tests: A meta-analytic review. Assessment, 2, 319– 331.
- Bornstein, R.F. (1996a). Beyond orality: Toward an object relations/ interactionist reconceptualization of the etiology and dynamics of dependency. Psychoanalytic Psychology, 13, 177–203.
- Bornstein, R.F. (1996b). Construct validity of the Rorschach Oral Dependency Scale: 1967–1995. Psychological Assessment, 8, 200–205.
- Bornstein, R.F. (1997). Dependent personality disorder in the DSM-IV and beyond. Clinical Psychology: Science and Practice, 4, 175–187.
- Bornstein, R.F. (1998a). Implicit and self-attributed dependency needs in dependent and histrionic personality disorders. Journal of Personality Assessment, 71, 1–14.
- Bornstein, R.F. (1998b). Implicit and self-attributed dependency strivings: Differential relationships to laboratory and field measures of help-seeking. Journal of Personality and Social Psychology, 75, 778–787.
- Bornstein, R.F. (1999). Criterion validity of objective and projective dependency tests: A meta-analytic assessment of behavioral prediction. Psychological Assessment, 11, 48–57.
- Bornstein, R.F. (2002). A process dissociation approach to objective-projective test score interrelationships. Journal of Personality Assessment, 78, 47–68.
- Bornstein, R.F., Bonner, S., Kildow, A.M., & McCall, C.A. (1997). Effects of individual versus group test administration on
Rorschach Oral Dependency scores. Journal of Personality Assessment, 69, 215–228.
- Bornstein, R.F., Bowers, K.S., & Bonner, S. (1996a). Effects of induced mood states on objective and projective dependency scores. Journal of Personality Assessment, 67, 324–340.
- Bornstein, R.F., Bowers, K.S., & Bonner, S. (1996b). Relationships of objective and projective dependency scores to sex role orientation in college students. Journal of Personality Assessment, 66, 555–568.
- Bornstein, R.F., Hilsenroth, M.J., Padawer, J.R., & Fowler, J.C. (2000). Interpersonal dependency and personality pathology: Variations in Rorschach Oral Dependency scores across Axis II diagnoses. Journal of Personality Assessment, 75, 478–491.
- Bornstein, R.F., & O’Neill, R.M. (1997). Construct validity of the Rorschach Oral Dependency (ROD) Scale: Relationship of ROD scores to WAIS-R scores in a psychiatric inpatient sample. Journal of Clinical Psychology, 53, 99–105.
- Bornstein, R.F., Riggs, J.M., Hill, E.L., & Calabrese, C. (1996). Activity, passivity, self-denigration, and self-promotion: Toward an interactionist model of interpersonal dependency. Journal of Personality, 64, 637–673.
- Bornstein, R.F., Rossner, S.C., & Hill, E.L. (1994). Retest reliability of scores on objective and projective measures of dependency. Journal of Personality Assessment, 62, 398–415.
- Bornstein, R.F., Rossner, S.C., Hill, E.L., & Stepanian, M.L. (1994). Face validity and fakability of objective and projective measures of dependency. Journal of Personality Assessment, 63, 363–386.
- Cohen, J. (1977). Statistical power analysis for the behavioral sciences. New York: McGraw-Hill.
- Dawes, R.M. (1994). House of cards: Psychology and psychotherapy built on myth. New York: Free Press.
- Fisher, J.M., & Fisher, S. (1975). Response to cigarette deprivation as a function of oral fantasy. Journal of Personality Assessment, 39, 381–385.
- Fisher, S. (1970). Body experience in fantasy and behavior. New York: Appleton-Century-Crofts.
- Fowler, J.C., Hilsenroth, M.J., & Handler, L. (1996). A multimethod approach to assessing dependency: The Early Memory Dependency Probe. Journal of Personality Assessment, 67, 399–413.
- Fowler, J.C., Hilsenroth, M.J., & Handler, L. (2000). Martin Mayman’s early memories technique: Bridging the gap between personality assessment and psychotherapy. Journal of Personality Assessment, 75, 18–32.
- Freud, S. (1905). Three essays on the theory of sexuality (Standard Ed., Vol. 7, pp. 125–248). London: Hogarth.
- Goldman-Eisler, F. (1950). The etiology of the oral character in psychoanalytic theory. Journal of Personality, 19, 189–196.
- Heathers, G. (1955). Acquiring dependence and independence: A theoretical orientation. Journal of Genetic Psychology, 87, 277– 291.
- Hill, E.F. (1972). The Holtzman Inkblot Technique. San Francisco: Jossey-Bass.
- Hirschfeld, R.M.A., Klerman, G.L., Gough, H.G., Barrett, J., Korchin, S.J., & Chodoff, P. (1977). A measure of interpersonal dependency. Journal of Personality Assessment, 41, 610–618.
- Holtzman, W.H. (1961). Guide to administration and scoring: Holtzman Inkblot Technique. New York: Psychological Corporation.
- Hunsley, J., & Bailey, J.M. (1999). The clinical utility of the Rorschach: Unfulfilled promises and an uncertain future. Psychological Assessment, 11, 266–277.
- Kagan, J., & Mussen, P. (1956). Dependency themes on the TAT and group conformity. Journal of Consulting Psychology, 20, 29–32.
- Karliner, R., Westrich, E., Shedler, J., & Mayman, M. (1996). The Adelphi Early Memory Index: Bridging the gap between psychodynamic and scientific psychology. In J.M. Masling & R.F. Bornstein (Eds.), Psychoanalytic perspectives on developmental psychology (pp. 43–67). Washington, DC: American Psychological Association.
- Lanyon, R.I., & Goodstein, L.D. (1997). Personality assessment. New York: Wiley.
- Lazare, A., Klerman, G.L., & Armor, D.J. (1966). Oral, obsessive, and hysterical personality patterns. Archives of General Psychiatry, 14, 624–630.
- Leichsenring, F. (1991). Discriminating schizophrenics from borderline patients: Study with the Holtzman Inkblot Technique. Psychopathology, 24, 225–231.
- Lilienfeld, S.O., Wood, J.M., & Garb, H.N. (2000). The scientific status of projective techniques. Psychological Science in the Public Interest, 1, 27–66.
- Masling, J.M. (1960). The influence of situational and interpersonal variables in projective testing. Psychological Bulletin, 57, 65–85.
- Masling, J.M. (1986). Orality, pathology, and interpersonal behavior. In J.M. Masling (Ed.), Empirical studies of psychoanalytic theories (Vol. 2, pp. 73–106). Hillsdale, NJ: Erlbaum.
- Masling, J.M., Rabie, L., & Blondheim, S.H. (1967). Obesity, level of aspiration, and Rorschach and TAT measures of oral dependence. Journal of Consulting Psychology, 31, 233–239.
- Mayman, M. (1968). Early memories and character structure. Journal of Projective Techniques and Personality Assessment, 32, 303–316.
- McClelland, D.C., Koestner, R., & Weinberger, J. (1989). How do self-attributed and implicit motives differ? Psychological Review, 96, 690–702.
- Meyer, G.J. (1996). The Rorschach and MMPI: Toward a more scientific understanding of cross-method assessment. Journal of Personality Assessment, 67, 558–578.
- Meyer, G.J., & Handler, L. (1997). The ability of the Rorschach to predict subsequent outcome: A meta-analysis of the Rorschach Prognostic Rating Scale. Journal of Personality Assessment, 69, 1–38.
- Millon, T. (1996). Disorders of personality: DSM-IV and beyond. New York: Wiley.
484 Projective Assessment of Interpersonal Dependency
- Mischel, W., & Shoda, Y. (1995). A cognitive-affective system theory of personality: Reconceptualizing situations, dispositions, dynamics, and invariance in personality structure. Psychological Review, 102, 246–268.
- Murray, H. (1938). Explorations in personality. New York: Oxford University Press.
- Nevo, B. (1985). Face validity revisited. Journal of Educational Measurement, 22, 287–293.
- Nevo, B., & Svez, J. (1985). Examinees’ feedback questionnaires. Assessment and Evaluation in Higher Education, 10, 236–249.
- O’Neill, R.M., Greenberg, R.P., & Fisher, S. (1984). Orality and field dependence. Psychoanalytic Psychology, 1, 335–344.
- Pincus, A.L., & Gurtman, M.B. (1995). The three faces of interpersonal dependency: Structural analysis of self-report dependency measures. Journal of Personality and Social Psychology, 69, 744–758.
- Rosenthal, R. (1966). Experimenter effects in behavioral research. New York: Appleton-Century-Crofts.
- Sappenfield, B.R. (1965). Review of the Blacky Pictures. In O.K. Buros (Ed.), Sixth mental measurements yearbook (pp. 1221– 1228). Highland Park, NJ: Gryphon Press.
- Sattler, J.M., & Winget, B.M. (1970). Intelligence testing procedures as affected by expectancy and IQ. Journal of Clinical Psychology, 26, 446–448.
- Schafer, R. (1954). Psychoanalytic interpretation in Rorschach testing. New York: Grune & Stratton.
- Sears, R.R., Rau, L., & Alpert, R. (1965). Identification and child rearing. Evanston, IL: Row-Peterson.
- Sinha, J.B.P. (1968). A test of dependence proneness. Journal of Psychological Research, 12, 66–70.
- Viglione, D.J. (1999). A review of recent research addressing the utility of the Rorschach. Psychological Assessment, 11, 251– 265.
- Wagner, E.E. (1983). The Hand Test: Manual for administration, scoring, and interpretation. Los Angeles: Western Psychological Services.
- Walters, R.H., & Parke, R.D. (1964). Social motivation, dependency, and susceptibility to social influence. In L. Berkowitz (Ed.), Advances in experimental social psychology (Vol. 1, pp. 231–276). New York: Academic Press.
- Weiner, I.B. (2000). Using the Rorschach properly in practice and research. Journal of Clinical Psychology, 56, 435–438.
- Weiss, L.R. (1969). Effects of subject, experimenter, and task variables on compliance with the experimenter’s expectation. Journal of Projective Techniques and Personality Assessment, 33, 247–256.
- Wood, J.M., Lilienfeld, S.O., Garb, H.N., & Nezworski, M.T. (2000). The Rorschach Test in clinical diagnosis: A critical review, with a backward look at Garfield (1947). Journal of Clinical Psychology, 56, 395–430.
- Zuckerman, M., & Grosz, H.J. (1958). Suggestibility and dependency. Journal of Consulting Psychology, 22, 328.
Projective Assessment of Borderline Psychopathology
MARK A. BLAIS AND KIMBERLY BISTIS
ASSESSING THOUGHT DISTURBANCE AND REALITY CONTACT 486
ASSESSING A VULNERABILITY TO PSYCHOTIC EXPERIENCE 486
- THE ASSESSMENT OF REALITY CONTACT USING TRADITIONAL RORSCHACH VARIABLES 488
- REALITY CONTACT AND THE THEMATIC APPERCEPTION TEST 489
- PROJECTIVE ASSESSMENT OF OBJECT-RELATIONS PHENOMENA 490
- PROJECTIVE ASSESSMENT OF DEFENSIVE FUNCTIONING IN BORDERLINE PSYCHOPATHOLOGY 492
It has been argued that no definitive projective assessment profile of patients with borderline psychopathology (BP) or borderline personality disorder (BPD) exists (J. Murray, 1993). However, the ability of projective assessment to assist in describing, diagnosing, and treatment planning for patients with BP is well established (Acklin, 1993; Exner, 1986b; Gartner, Hurt, & Gartner, 1989; Hurt, Reznikoff, & Clarkin, 1991; P. Lerner, 1991). The diversity and richness of projective data relevant to BP is impressive and comes from multiple sources such as the Rorschach Inkblot test (Rorschach, 1942), Thematic Apperception Test (TAT; H.A. Murray, 1943), and Early Memories Test (Mayman, 1968), as well as other projective techniques. In this chapter we will review the recent empirical and clinical writings relevant to utility of projective data for assessment of BP. The review will focus mainly on research involving the major projective assessment techniques, the Rorschach and Thematic Apperception Test, as well as a lesser known technique, the Early Memories Test. The chapter will conclude by integrating these data into a coherent summary that may serve to enhance clinical work as well as ongoing empirical research and theory development.
AGGRESSION AND BORDERLINE PSYCHOPATHOLOGY 494 BOUNDARY DISTURBANCE AND BORDERLINE PSYCHOPATHOLOGY 495 ASSESSING THE SEVERITY OF BORDERLINE PSYCHOPATHOLOGY 495 CONCLUSIONS 496 NOTES 497 REFERENCES 497
The inclusion of Axis II in the 3rd edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-III; American Psychiatric Association, 1980), with its focus on personality (features and disorders), invigorated personality assessment research in general and particularly the study of BPD. In fact, since the introduction of the DSM-III, BPD has been the most frequently studied personality disorder (Gunderson, 2001). In the current DSM (4th ed. [DSM-IV]; American Psychiatric Association, 1994), BPD is identified by nine criteria (see Table 36.1) reflecting the four essential features of the disorder: instability of interpersonal relationships, self-image, affects, and marked impulsivity. To qualify for a diagnosis of BPD a patient must exhibit at least five of these nine criteria. Although successive revisions of the DSM
TABLE 36.1 DSM-IV Borderline Personality Disorder Criteria
- Frantic efforts to avoid abandonment
- Unstable relationships
- Identity disturbance
- Impulsivity
- Suicidal behavior
- Affective instability
- Feeling empty
- Intense anger
- Transient paranoid or dissociative symptoms
Note. Criteria adapted from the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (APA, 1994).
Acknowledgements: MAB would like to thank RR-V and MJH for their support and helpful comments during the writing of this paper.
have improved the clarity and reliability of this disorder (Blais, Hilsenroth, & Castlebury, 1997; Blais, Hilsenroth, & Fowler, 1999; Blais, Kelly, Holdwick, & Hilsenroth, 2001), the current diagnostic algorithm produces over 200 variations, making the DSM-IV BPD a broad and heterogeneous disorder.
While BPD may be a recent addition to the official psychiatric nomenclature, the concepts of borderline personality and borderline psychopathology are not new (Gunderson, 2001). In fact, to a considerable degree, the earlier psychoanalytic concepts of Borderline States (Knight, 1953) and then Borderline Personality Organization (BPO, Kernberg, 1975) laid the foundation for the DSM BPD. In writing about borderline states, Knight highlighted the fact that these patients evidenced severe, nonspecific ego weaknesses including brief periods of poor reality contact and a propensity for regression in unstructured settings, despite initially appearing to be more psychologically intact. Kernberg (1970, 1975) advanced our understanding of these patients by developing a complex hierarchical psychoanalytic model of personality development and organization. Kernberg’s model places personality development on a continuum of functioning that runs from the lower psychotic pole through borderline to the higher neurotic pole. BPO represents a large middle range of psychological development within Kernberg’s model. This broad developmental area is marked by identity diffusion, disturbances in object relations, lapses in reality contact, and reliance on primitive defenses, such as splitting and projection and excessive aggression. However, given that Kernberg’s concept of BPO is bounded on one end by psychotic organization and on the other by neurotic organization, the range of pathology evidenced by patients falling within Kernberg’s borderline group is substantial. Kernberg’s theory of personality and his ideas regarding BPO continue to be influential among psychodynamically oriented psycho-diagnosticians and therapists (P. Lerner, 1991).
As a result of their different developmental lines two related and somewhat overlapping conceptualizations of BP currently coexist in the professional literature. However, despite the differences in their origins and diagnostic emphases (BPD external behavior, BPO internal experience) the two versions of BP may be more alike than they are different. Both versions of BP reflect broad heterogeneous conceptualizations allowing for considerable cross-system overlap. Additionally, the two versions of BP share a number of important core features. For example, the DSM-IV BPD and Kernberg’s BPO focus on disrupted relationships (DSM-IV BPD Criteria 1, 2, and 7), underdeveloped identity (BPD Criterion 3), poor affect regulation and trouble controlling anger (BPD Criteria 6 and 8), and occasional lapses in reality contact (BPD Criterion 9). Factor analysis of the DSM-IV BPD criteria set identified a large first factor that reflected difficulties with self-other differentiation and boundary disturbance (Blais et al., 1997), perhaps the core feature of BP in Kernberg’s model. Not surprisingly, in a study comparing different diagnostic measures of borderline personality, Lewis and Harder (1991) found a significant degree of overlap between patients diagnosed as (Kernberg’s) BPO and those diagnosed with the DSM-III-R BPD (3rd ed. revised [DSM-III-R]; American Psychiatric Association, 1986). In fact, Kernberg’s Structural Interview diagnosis of BPO and the DSM-III-R diagnosis of BPD were in agreement on 82% of the cases (Lewis & Harder, 1991). Given that such a high degree of agreement has been shown to exist both empirically and conceptually between these two versions of borderline psychopathology, they will be treated without formal distinction in this review. From the material reviewed above, a number of areas of functioning appear to be particularly relevant to the projective assessment of BP: reality testing, boundary disturbances, object relations, defensive functioning, and control of anger or aggression.
ASSESSING A VULNERABILITY TO PSYCHOTIC EXPERIENCE
Both the DSM-IV and Kernberg’s models of borderline psychopathology suggest that borderline patients have a vulnerability to experiencing brief episodes of psychotic phenomena. Clinical lore based on Rapaport’s (Rapaport, Gill, & Schaefer, 1968) observations regarding the test performance of preschizophrenic patients holds that such a vulnerability to psychotic experience is observable on full battery testing. It is believed that borderline patients demonstrate their vulnerability to psychosis by producing clear signs of mild thought disturbance on the Rorschach, while producing “clean” (nonthought-disordered) Wechsler Adult Intelligence Scale (WAIS; Wechsler, 1981) protocols. This pattern of test results, namely a disturbed Rorschach and clean WAIS, has also been interpreted as a reflection of the borderline patient’s lack of internal psychological structure and his or her need for external structure to achieve adequate adaptive functioning. Through the ’50s, ’60s, and ’70s, the belief in this assertion was so strong that findings of such a pattern were taken as being axiomatic of a borderline diagnosis (Kleiger, 1999).
Widiger (1982) performed one of the first reviews of the Rorschach-WAIS thought disturbance literature. He concluded that there was not adequate empirical support for the widely held view that borderline patients produced disturbed Rorschachs and clean WAISs. Widiger also provided suggestions for improving research in this area. Research exploring the differential production of thought disturbance cross-tests requires valid and reliable systems for quantifying the degree of thought disturbance present in verbal material, independent of how the verbal material was generated. The Thought Disorder Index or TDI (Johnston & Holzman, 1979), a scale that grew out of Rapaport’s (1968) initial efforts to systematically evaluate the quality of thought, is one of the most widely employed scales of this type. O’Connell, Cooper, Perry, and Hoke (1989) found that in a mixed group of inpatients, TDI scores of admission Rorschach responses predicted the later appearance of psychotic symptoms better than
a structured psychiatric interview. Recently Kircher et al. (2001) successfully used functional magnetic resonance imaging (fMRI) and Rorschach-derived TDI scores to identify the neural-anatomical correlates of formal thought disorder. Both of these studies highlight the excellent validity of the TDI as a measure of thought disturbance. Since its development the TDI has been used in a number of studies seeking to compare the degree of thought disorder present across various test protocols.Table 36.2 provides an outline of the TDI scoring system.
Reviewing the literature that developed following Widiger’s critique and the development of scoring systems like the TDI, Gartner et al. (1989) concluded that borderline patients produced signs of moderately severe thought disturbance across all psychological tests, including the WAIS. However, they felt that the accumulated research supported the idea that the degree of thought disturbance of borderline patients seen on the WAIS was less than that produced on the WAIS by psychotic patients. In contrast, borderline and psychotic patients tended to produce equal signs of thought disturbance on the Rorschach. More recently, Harris (1993), using the TDI, found that borderline outpatients did not differ from other personality disorder outpatients in the degree of thought disorder shown on the WAIS. However, they did produce significantly more mild and moderately severe signs of thought disturbance on the Rorschach. While noting that the borderline patients in her study did not produce “clean” WAIS protocols, Harris concluded that “the empirical results supported the clinical observation that borderlines demonstrate greater evidence of thought disorder, particularly in unstructured situations” (Harris, 1993, p. 117).
A strikingly similar pattern of findings was reported Skelton, Boik, and Madero (1995) in their exploration of
| ———— |
– |
——————————————————- |
– |
– |
– |
|
.25
Minor, Rarely
Noticed |
.50
Intermediate but
Noticeable |
.75
Clear Thought
Disturbance |
1.0
Complete Loss of
Reality Contact |
|
Categories that can
be scored for each
level of severity |
Inappropriate
Distance
Flippant Responses
Vagueness
Peculiar
Verbalizations
and Responses
Word-Finding
Difficulties
Clangs
Perseveration
Incongruous
Combinations |
Relationship
Verbalizations
Idiosyncratic
Symbolism
Queer Responses
Confusion
Looseness
Fabulized
Combinations
Playful
Combinations
Fragmentation |
Fluidity
Absurd Responses
Confabulation
Autistic Logic |
Contamination
Incoherence
Neologisms |
|
thought disturbance on WAIS and Rorschach protocols of identity-disordered adolescents. Again using the TDI, they found that identity-disordered adolescents (thought by many to be an early version of BPD) showed greater discrepancy between the degree of thought disturbance on the WAIS and Rorschach than did comparison groups of conduct-disordered, defiant-disordered, and schizophreniform-disordered adolescents. These findings were maintained when response productivity and demographic variables were controlled for.
Taken together, the accumulated data do appear to provide at least partial support for the old clinical belief regarding the discrepancy between the degree of thought disturbance seen on the WAIS and Rorschach of borderline patients. However, the magnitude of these findings varies depending upon the comparison groups used in the studies. For example, it appears that WAISs of borderline patients are “cleaner” than the WAISs of psychotic patients but are not always “cleaner” than other PD groups. Also, the Rorschachs of borderline patients show more signs of thought disturbance than do the Rorschachs of nonpatients and other personality disorder patients. Still, it is also likely that the majority of borderline patients will produce some evidence of thought disturbance on the WAIS (Harris, 1993).
THE ASSESSMENT OF REALITY CONTACT USING TRADITIONAL RORSCHACH VARIABLES
In the Comprehensive System (CS; Exner, 1986a, 1993), thought quality and reality contact roughly correspond to Form Quality (X and F percentages) reflecting perceptual accuracy and the Sum6 along with specific Special Scores tapping quality of thinking. In addition, the CS Schizophrenia Index (SCZI) has proven valuable for evaluating the quality of thought and likely presence of psychosis contained within a Rorschach protocol.
In one of the earliest studies of borderline patients using the CS, Exner (1978) compared the protocols of 21 expertly diagnosed borderlines to those of 25 “remitted” schizophrenics. A number of interesting similarities and differences were noted between the groups. The two groups were similar in F# and X# percentages, but the schizophrenics produced significantly more poor form responses (!), while the borderline patients produced more weak form responses (u). Schizophrenics produced more M!, while borderline protocols contained significantly more Texture (T) and Space (S) responses. The schizophrenic group had an average of 3.9 Special Scores compared to 1.6 for the borderline group. From these findings, Exner concluded, “borderlines display a Rorschach structure that can easily be identified as representing the very inadequate or very immature personality. They are angry, very self-centered, have poor emotional controls, bend reality to fit their own uniqueness . . .” (Exner, 1978, p. 252).
Regarding the quality of borderline thinking, Rapaport et al. (1968) again provides the starting point. Rapaport observed that “overideational preschizophrenics” (a heterogeneous diagnostic group that would include many of today’s borderlines) tended to produce more moderate signs of thought disturbance. Typically these patients produced fabulized1 responses and fabulized combinations (FABCOMs) rather than confabulized responses, which are thought to reflect more severe thought disturbance. As Kleiger (1999) nicely summarized in his book on disordered thinking and the Rorschach, a number of early Rorschach studies found empirical support for Rapaport’s position. In fact, the findings from three of these studies showed substantial convergence. Patrick and Wolfe (1983); Singer and Larson (1981); and Steiner, Martin, Wallace, and Goldman (1984) all found surprisingly similar rates for fabulized combinations. Across these three studies the percentage of borderline patients that produced protocols with two or more fabulized combinations ranged from 57 to 64.
Exner (1986b) compared the Rorschach protocols of borderline, schizotypal, and schizophrenic subjects on a number of variables related to thought disturbance. Over half (56%) of the borderline subjects produced one or more incongruous combination (INCOM) responses. An INCOM response is a form of combinatory thinking in which blot images or details are merged into a single image in an inappropriate manner (this is thought to reflect a mild form of thought disturbance). Over 70% of the schizophrenic subjects in Exner’s study gave at least one INCOM response. Consistent with his earlier study, Exner also found that the schizophrenic group produced more poor or minus form responses (X! and F!) than did the borderline group.
Research has consistently reported borderline patients achieving Rorschach Form Quality scores (X# and F# percentages) ranging from 65 to 70 (Gartner, Hurt, & Gartner, 1989; Kleiger, 1999). This would place the Form Quality achieved by borderline patients nicely between that of schizophrenic subjects (who score about 10 points lower) and nonpatients (who score 5 to 10 points higher).
A recent study exploring the psychometric quality of the Rorschach Schizophrenia Index (SCZI; Hilsenroth, Fowler, & Padawer, 1998) provides additional insights into the degree of thought disturbance evidenced by borderline patients. In this study, borderline patients had a mean SCZI of 3.0, which was significantly less than a group of psychotic patients (mean SCZI 4.5), but significantly greater than a group of Cluster C personality-disordered patients (SCZI ” 1.8) and
| Harris (1993) |
Rorschach
WAIS-R |
BPD produced ! TID scores on Rorschach but
not on the WAIS-R |
Other PDs |
| Exner (1978) |
Rorschach |
Fewer (–) form responses
More (u) form responses
Lower Special Score total |
Schizophrenics |
| Exner (1986b) |
Rorschach |
56% of BPD protocols had “1 INCOM
responses |
Schizophrenics
Schizotypals |
Gartner, Hurt, & Gartner
(1989) |
Rorschach |
X# and F# %s of BPD protocols range from
.65–.70 |
|
| Kleiger (1999) |
|
BPD X# 10 points ! schizophrenics and 5 to
10 ! than nonpatients |
|
Hilsenroth, Fowler, &
Padawer (1998) |
Rorschach |
Mean SCZI score for BPD subjects ” 3.0
Criteria 4 and 5 of SCZI met less frequently for
BPD subjects |
Schizophrenics
Nonpatients
Cluster C PDs |
| Westen et al. (1985) |
TAT |
BPD subjects have low score on the Social
Causality scale of the SCORS |
Major depression |
TABLE 36.3 Selected Summary of the Literature on Borderline Psychopathology and Thought Disturbance
a nonclinical group (SCZI ” 1.1). Furthermore, in this study the Special Score (SS) markers of severe thought disturbance contained in the SCZI proved to be “especially useful” in differentiation between the psychotic and borderline groups. Fewer borderline patients satisfied SCZI Criteria 4 (sum level 2 SS ! 1 and FAB2 ! 0) or Criteria 5 (raw Sum6 # 6 or Wsum6 ! 17) than did psychotic subjects.
Looking across these studies (see Table 36.3) it seems reasonable to accept the commonly held notion that borderline patients will frequently produce a couple of signs of mild to moderate thought disturbance on the Rorschach. However, the amount of thought disturbance evident in the borderline patient’s Rorschach will usually be less than that seen in the Rorschachs of schizophrenic patients. Unlike schizophrenic subjects, when borderlines do misperceive the form of the Rorschach stimuli, it will usually be a weak “violation” of form quality (Xu) rather than a severe violation (X!). The nature of the borderline thought disturbance will also be mild to moderate typically reflected in INCOM, DR, and FAB-COM Level 1 Special Scores. It can be said that borderlines perceive reality with reasonably good accuracy, but misinterpret their perceptions based upon idiosyncratic needs or overvalued ideas.
REALITY CONTACT AND THE THEMATIC APPERCEPTION TEST
Although it is one of the most widely used clinical assessment tools, the status of the Thematic Apperception Test (H.A. Murray, 1943) has often been questioned as it lacks a standardized administration method, a reliable scoring system, and an adequate normative sample. Still, a number of more circumscribed scoring systems for the TAT have been developed, such as Cramer’s system for scoring Defensive Mechanisms (Cramer, 1999) and Westen’s Social Cognition and Object Relations Scale (SCORS; Westen, Lohr, Silk, Kerber, & Goodrich, 1985). Both systems have demonstrated adequate reliability and validity to support their clinical and research application. Given the more subtle nature of the borderline patient’s vulnerability to psychosis, it would be unrealistic to expect florid signs of psychosis on the more structured TAT, especially if such severe signs are not typically encountered on the Rorschach. However, one of the scales from Westen’s SCORS, the Social Causality subscale, does appear to be sensitive to the borderline patient’s vulnerability to mild disruptions in reality contact.
As defined by Westen (Westen et al., 1985), the SCORS Social Causality scale measures the extent to which attributions about the causes of people’s actions, thoughts, and feelings are logical and accurate. Low scores on this scale reflect inaccurate and illogical causal inferences regarding motives, actions, and feelings of others. As Westen (1990) has indicated, “clinical experience with severe personality disorders suggests that these patients tend to make highly idiosyncratic, illogical and inaccurate attributions of people’s intentions” (p. 679). Westen further suggests that limitations in this area may reflect a structural and cognitively based difficulty in generating accurate social attributions. Such a deficit is likely the case with many schizoid and borderline patients who read people poorly and illogically, even when there is minimal psychological need to distort (Westen, 1990).
Given that the Social Causality scale of the SCORS focuses on the degree of logic and accuracy present in a patient’s interpretation of social interactions, it might serve as an additional measure of the types of mild to moderate thought disturbance produced by borderline patients. The research to date has been somewhat mixed in this area. In a series of studies with both adult and adolescent borderline subjects, Westen and colleagues (Westen Lohr, Silk, Gold, & Kerber, 1990; Westen, Ludolph, Lerner, Ruffins, & Wiss, 1990) found that borderline patients, among other things, produced “grossly illogical attributions.” In summarizing all the SCORS studies existent at that time (not limited to those using the TAT), Westen concluded “Borderlines . . . tend to attribute the causes of other people’s behavior, thoughts, and feelings in idiosyncratic ways” (Westen, 1990, p. 682). A recent study by Ackerman, Clemence, Weatherill, and Hilsenroth (1999) partly confirms Westen’s conclusion. The findings from the Ackerman et al. study (see their Table 3, p. 433) showed that the borderline subjects scored significantly lower on the SCORS Social Causality subscale than did a group of narcissistic PD subjects. The borderline group was also lower, but not at the level of statistical significance, than a group of mixed Cluster C personality disorder subjects (mean score 3.86, SD .53 for BPD and mean 4.03, SD .58 Cluster C PDs). While somewhat mixed and requiring additional empirical study, these findings suggest that the application of Westen’s SCORS (particularly the Social Causality subscale) to TAT stories may provide additional information regarding the quality of thinking in borderline subjects.
PROJECTIVE ASSESSMENT OF OBJECT-RELATIONS PHENOMENA
Although not identical in their conceptualizations, disrupted or conflicted object relations are a central feature of borderline psychopathology in both the DSM and Kernberg’s diagnostic systems. The DSM, with its behavioral emphasis, makes the instability evidenced in the borderline patient’s external relationships a prime focus, while Kernberg’s psychoanalytic conceptualization focuses on deficits in the borderline patient’s internalized object representations. While a number of projective assessment techniques including the Rorschach, TAT (H.A. Murray, 1943), and Early Memories Test (EMT; Mayman, 1968) have proven valuable in evaluating the object relations of borderline patients, the usefulness of the TAT stands out in this area. In fact, Westen (1990, 1991) has argued that the TAT, with its moderately ambiguous drawings of human figures in various emotional and interpersonal situations, is uniquely suited among psychological tests for eliciting information regarding a patient’s object relations. In addition, Westen (1990) has developed a reliable and valid multidimensional measure of object relations that is well suited to scoring the quality of object relations de-
| ———— |
————————————————————– |
– |
– |
– |
– |
| SCORS categories |
1 |
5 |
7 |
Complexity of
representations |
Egocentric
representations |
Conventional
representations |
Differentiated and
complex
representations |
Affective quality of
representations |
Malevolent and abusive |
Mixed positive and
negative |
Mostly positive |
Emotional investment in
representations |
Self/need focused |
Mixed focus on needs |
Focus on meeting mutual
needs |
Investment in values and
morals |
Self-indulgent and
remorseless |
Invested in and tries to
meet moral values |
Thoughtful and
compassionate,
challenges convention |
Understanding social
causality (SC) |
Confused and unusual
view of SC |
Straightforward view of
SC |
Complex and coherent
view of mutual SC |
Experiencing and
managing aggression |
Physically assaultive and
destructive |
Denies anger and avoids
confrontations |
Assertive and appropriate
expression of anger |
| Self-esteem |
Evil, loathsome self
image |
Range of self-image with
positive and negative |
Realistic positive self
image |
Identity and coherence of
self |
Fragmented sense of self |
Adequately stable
identity and sense of
self |
Integrated sense of self
with long-range goals
and plans |
picted in TAT stories. Table 36.4 presents a brief summary of the categories and range of object-relations phenomena tapped by Westen’s Social Cognition and Object Relations Scale (SCORS, see Table 36.4).
Westen et al. (1990) used the SCORS to rate the objectrelations themes present in the TAT stories of patients with BPD, major depressive disorder (MDD), and nonclinical controls. Their findings showed that compared to the nonclinical control group, BPD subjects had lower mean scores on complexity, affective tone, capacity for emotional investment, and understanding social causality. The BPD subjects also saw relationships and others as being more malevolent than did the MDD group.
Recently, Ackerman et al. (1999) used a revised and expanded version of the SCORS to explore the object relations of the DSM-IV Cluster B personality disorders (Cluster B PDs) and a comparison group of Cluster C personality disorders (Cluster C PDs) as they were revealed in TAT stories. In this study, the subjects with BPD had significantly lower scores on four of the eight SCORS scales (Affective Tone, Morals, Aggression, and Identity) than did the Cluster C PD subjects. Compared to Narcissistic PD, (NPD, another Cluster B PD) the BPD group produced significantly lower (more pathological) scores on all eight of the SCORS categories. This finding is consistent with previous research indicating that patients with BPD tend to be more impaired than patients with NPD. While the Cluster B Antisocial PD (ANPD) and BPD were indistinguishable based on mean SCORS ratings, multiple regression analysis showed that the two disorders were differentially predicted by the SCORS scales. BPD was predicted by Affective Tone (Standardized Coefficient [SC] of !.47, Step 1) and Investment in Relationships (SC .14, Step 2), while ANPD was predicted by Investment in Relationships (SC !.48, Step 1) and Affective Tone (SC .40, Step 2). This finding suggests that the BPD subjects saw their relationships as more malevolent and negative, but had investment in maintaining them, whereas the ANPD subjects had little investment in maintaining their relationships, but did not see others as being malevolent.
While the TAT may be well suited to assessing object relations, both the Rorschach and the EMT (Mayman, 1968) have also proven useful in evaluating the object world of BPD patients. The Rorschach assessment of object relations can be greatly facilitated by the use of the Urist Mutuality of Autonomy Scale (MOAS; Urist, 1977). The MOAS (see Table 36.5) was developed to assess various stages or levels of interpersonal relatedness. Using a 7-point scale the MOAS rates the quality of relationships depicted in Rorschach responses. The relationship may be between either animate (human or animal) or inanimate objects. Lower MOAS scores (1, 2, and 3) reflect more mature and developmentally advanced relationships, while higher scores (5, 6, and 7) reflect more negative and primitive relationships.
Blais and colleagues (Blais, Hilsenroth, Fowler, & Conboy, 1999; Blais, Hilsenroth, Castlebury, Fowler, & Baity, 2001) have shown that the Rorschach responses of borderline patients frequently depict highly pathological relationships as rated by the MOAS. In a study exploring the Rorschach profiles of the DSM-IV Cluster B personality disorders, Blais, Hilsenroth, Fowler, & Conboy (1999) found that the highest (most pathological) MOAS score (MOAS-H) was significantly correlated with BPD, but with no other Cluster B PD. In addition, the Rorschach Oral Dependency Scale (ROD; Masling, Rabie, & Blondheim, 1967), a measure of dependency needs, was significantly, but negatively, correlated with BPD criteria.2 Further analyses revealed that MOAS-H was significantly related to two of the three core features of the DSM-IV BPD while ROD was associated with all three. These findings suggest that negative, developmentally primitive relationships that are permeated with overcontrolled dependency needs (insecure attachment style) are core interpersonal relational aspects of BPD.
In a second study, Blais et al. (2001) demonstrated the incremental validity of Rorschach variables over the Minnesota Multiphasic Personality Inventory-2 (MMPI-2; Butcher, Dahlstrom, Graham, Tellegen, & Kaemmer, 1989) Personality Disorder scales (Colligan, Morey, & Offord, 1994) for predicting DSM-IV Cluster B PD criteria, including BPD. In
TABLE 36.5 The Urist Mutuality of Autonomy Scale (MOAS)
| Developmental level |
Mutual mature |
Dependent and mirroring |
Primitive merger-based |
|
relationships |
relationships |
relationships |
| Degree of differentiation |
Well-maintained self–
other representations |
Blending of boundaries |
Nearly complete
de-differentiation with
malevolence |
| Sample Rorschach |
Two people talking at a |
Siamese twins connected |
An evil fog engulfing |
| response |
party |
at the waist |
something smothering it |
| Urist (1977) |
Rorschach |
BPD protocols have ! MOAS scores of
5,6,7 |
|
Blais et al.
(1999) |
Rorschach |
Highest MOAS score correlates with
BPD |
Other Cluster B PDs |
Blais et al.
(1999) |
Rorschach |
ROD scores are negatively correlated
with BPD |
Other Cluster B PDs |
Westen et al.
(1985) |
TAT |
BPD subjects have lower mean scores
on the SCORS scales of Complexity,
Affective Tone, Capacity for
Emotional Investment, Understanding
of Social Causality |
Major depressive
disorder and
nonpatients |
Fowler et al.
(2000) |
Rorschach |
Self-mutilating BPD subjects had more
impaired object relations on MOAS |
Non-self-mutilating BPD |
Ackerman et al.
(1999) |
TAT |
BPD subjects had lower scores on all
eight scales of the SCORS |
Narcissistic PD |
Arnow &
Harrison
(1991) |
Early Memories Test |
BPD subjects had fewer positive
affective early memories
BPD subjects had the most negatively
toned memories |
Schizophrenics, neurotics |
Nigg et al.
(1992) |
Early Memories Test |
BPD subjects had more malevolent and
hurtful objects |
Major depressive
disorder |
TABLE 36.6 Selected Summary of the Literature on Borderline Psychopathology and Object Relations
this study Blais et al. (2001) found that after the MMPI-2 Borderline scale was forced into a regression equation at Step 1, both MOAS-H and ROD entered into the prediction of BPD criteria at Step 2. These findings provide evidence that Rorschach variables capture information relevant to interpersonal function that is not available from the self-report of borderline subjects (at least not when limited to the MMPI-2 item pool).
The EMT asks subjects to talk about a number of different early memories, including their earliest and next earliest memory, earliest memory of mother, earliest memory of father, and happiest and unhappiest memory. In addition, inquiries are typically made regarding the feeling tone of each memory reported. Arnow and Harrison (1991) found that the DSM-III borderline patients produced significantly fewer positive affective early memories than those of paranoid schizophrenics and a group of neurotics (defined as clinical subjects without severe psychopathology), while also producing the most negatively (opposed to neutral) toned memories. Nigg, Lohr, Westen, Gold, and Silk (1992) also used the EMT to explore the object world of borderline patients. When compared to the EMs of patients with MDD, the EMs of the borderline patients contained more malevolent and hurtful objects.
Overall, the findings from multiple studies using a variety of projective instruments are surprisingly consistent with regard to the object relations of borderline patients (see Table 36.6). These findings consistently reveal that borderline patients attribute more negative emotional qualities and more malevolent motives to others (and their internal representations of others) than do patients with other PDs or MDD. Interestingly, a recent experimental study of borderline patients provides support for the findings from the projective assessment studies reviewed. Arntz and Veen (2001) found that borderline patients rated film clips of interpersonal interactions as being more negative than did patients with Cluster C PDs. Furthermore, the tendency of borderline subjects to rate interactions negatively was more pronounced in what the researchers described as an unstructured format (Arntz & Veen, 2001).
PROJECTIVE ASSESSMENT OF DEFENSIVE FUNCTIONING IN BORDERLINE PSYCHOPATHOLOGY
According to Kernberg’s (1975) developmental model of character pathology, a specific level or configuration of defensive functioning marks BPO. In particular, Kernberg has theorized that patients with BPO should rely heavily upon the use of primitive defenses such as splitting, denial, idealization, devaluation, projection, and projective identification. Establishing the level of a patient’s defensive functioning is essential for making Kernberg’s BPO diagnosis. While level of defensive functioning is not directly considered in making a DSM-IV diagnosis of BPD, research has shown that the defensive functioning of DSM-IV borderline is highly consistent with Kernberg’s model (Blais, Conboy, Wilcox, & Norman, 1996). The projective assessment of defensive functioning has focused mainly on the application of defense scoring systems, like those of Cooper, Perry, and Arnow (1988) and P. Lerner and H. Lerner (1980).
Lerner and Lerner developed their Defense Scale (LDS; Lerner & Lerner, 1980) based upon Kernberg’s (1975) conceptualization of primitive defensives. The LDS operationalizes the defenses of splitting, idealizing, devaluing, denial, and projective identification, as these are depicted in human, quasi-human, and human detail Rorschach responses. Each of the specific defenses in the LDS is rated on a continuum from low (more pathological) to high (less pathological), reflecting the degree of distortion present. To use the scale, clinically or in research, the ratings for each specific defense are summed, yielding a total score for each defense. For example, if three instances of devaluation were identified and they were rated at the Levels of 3, 3, and 1, the patient would receive a total devaluation score of 7 (3#3#1 ” 7).
Gacono, Meloy, and Berg (1992) used the LDS to map the defensive operations of three groups of DSM PD patients: BPD, NPD, and ANPD. The findings from their study failed to reveal any differences between these three groups with regard to defensive functioning. All three groups relied heavily on primitive defenses. The authors suggested that the lack of between-group differences indicated that Kernberg would classify many patients from all three groups as BPO. However, in an earlier study utilizing the same BPD and NPD
sample as in Gacono et al. (1992), Berg (1990) found that the BPD group produced significantly more splitting responses than did the NPD group.
Hilsenroth, Hibbard, Nash, and Handler (1993) found that the LDS scales were useful in differentiating DSM-IV BPD patients from patients with both NPD and Cluster C PDs. Compared to NPD patients, the BPD group produced significantly more signs of splitting and projective identification. Blais, Hilsenroth, Fowler, and Conboy (1999) used three of the LDS defenses: splitting, projective identification, and devaluation in a Rorschach exploration of the Cluster B PDs. Using the total criteria per Cluster B PD as target variables (rather than specific diagnoses, given the high rates of comorbidity among PD patients), these researchers found the defenses of devaluation and splitting (but not projective identification) to be significantly associated with BPD. However, in this study, splitting also had significant positive correlation with the histrionic PD criteria (and was negatively correlated with NPD). The findings from Blais, Hilsenroth, Fowler, and Conboy (1999) reinforce the value of Rorschach data for identifying similarities and differences in the deeper psychological functioning of the DSM-IV PDs. In a follow-up study exploring the incremental validity of Rorschach variables relative to the MMPI-2 PD scales for predicting DSM-IV PD criteria, Blais et al. (2001) showed that the LDS defense of devaluation was an independent predictor of BPD criteria.
When taken together, these findings suggest that the projective assessment of defensive functioning can help identify patients with borderline psychopathology (see Table 36.7).
Gacono, Meloy, & Berg
(1992) |
Rorschach |
LDS scores not significantly different for BPDs |
Narcissistic PD
Antisocial PD |
| Hilsenroth et al. (1993) |
Rorschach |
BPD subjects score higher on LDS scales of
splitting and projective identification
BPD subjects score higher on PPA and SPA in
Holt system |
Narcissistic PD
Cluster C PD |
Blais, Hilsenroth, Fowler,
& Conboy (1999) |
Rorschach |
LDS scales of devaluation and splitting
associated with BPD |
Cluster BPDs |
| Blais et al. (2001) |
Rorschach |
LDS scale of devaluation is an independent
predictor of BPD |
Cluster BPDs |
| Gacono & Meloy (1994) |
Rorschach |
BPD subjects have more CS Aggressive
responses (mean”1.39) |
Narcissistic PD
Antisocial PD |
| Fowler et al. (2000) |
Rorschach |
Self-mutilating BPD subjects: More PPA in
Holt system
More defensive splitting, devaluing, and
idealizing on LDS |
Non-self-mutilating
BPDs |
| Ackerman et al. (1999) |
TAT |
BPD subjects have lower ratings on EMAI
subscale of the SCORS |
Narcissistic PD
Cluster C PD |
TABLE 36.7 Selected Summary of the Literature on Borderline Psychopathology and Defensive Functioning and Aggression
Furthermore, given their link to psycho-dynamic theory, these data can help describe specific aspects of functioning that have important implications for treatment. While a number of positive findings have been achieved using the LDS, some of these findings have been inconsistent. For example, projective identification has been associated with BPD in some studies (Hilsenroth et al., 1993) but not in others (Blais, Hilsenroth, Fowler, & Conboy, 1999). Also, while splitting has been associated with BPD (as theoretically predicted) it was also associated with HPD (Blais, Hilsenroth, Fowler, & Conboy, 1999; a finding that would be consistent with Kernberg’s model). At least one study (Gacono et al., 1992) failed to find any differences among groups of ANPD, NPD, and BPD subjects. While further research is needed to help clarify the meaning of these inconsistent findings, it is also likely that the mixed nature of these results, in part, reflects the inadequacies contained in the DSM system itself. It has been well established that the DSM-IV personality disorders do not represent clear, well-defined, and demarcated groups. At least within Cluster B, these disorders share many common features (Holdwick, Hilsenroth, Castlebury, & Blais, 1998), as Kernberg’s model would predict.
AGGRESSION AND BORDERLINE PSYCHOPATHOLOGY
Difficulties with the modulation and appropriate expression of anger and aggression are primary features in both the DSM-IV definition of BPD and Kernberg’s model of BPO. In the DSM diagnostic system, the focus is on identifying the presence of intense, inappropriate, and poorly controlled anger (see Criterion 8 in Table 36.1). Kernberg theorizes that the presence of excessive aggression early in life, either due to congenital or environmental factors, is a predisposing feature for developing BPO. Holt (1977) developed a method for assessing the quantity and quality of aggression present in verbal material. This method is based on the psychoanalytic concepts of primary and secondary process thinking and has been widely utilized in Rorschach research (Hilsenroth et al., 1993). Holt’s system identifies two forms of aggression, primary process aggression (PPA) and secondary process aggression (SPA). The hallmark of PPA is its raw, primitive, destructive, and murderous quality, while SPA reflects aggression or anger that is expressed in a more socially appropriate manner. To apply Holt’s system, Rorschach responses are reviewed for three categories of aggression: attack, victim, and outcome or results. Each instance of these categories is assigned a level of either PPA or SPA. Other systems for scoring aggression on the Rorschach include the coding of Aggressive Movement (Ag) in the CS and a system developed by Gacono and Meloy (1994) that codes for multiple aspects of aggression: aggressive content, aggression past, and aggressive potential. To date, Holt’s system has been the most widely studied. However, recent research has provided additional support for using a modified version of Gacono and Meloy’s system (see Baity & Hilsenroth, 1999; Baity, McDaniel, & Hilsenroth, 2000).
Hilsenroth et al. (1993) employed the Holt system for assessing aggression in their study of BPD, NPD, and Cluster C PDs. They found that BPD subjects produced significantly more PPA and SPA than did the Cluster C PDs. Interestingly, they also found that the BPD group produced more SPA than did the NPD group. The authors interpreted their findings as support for the presence of excessive aggression in BPD subjects and as indicating the range of expression that BPD aggression can take, from primitive to socially acceptable. Blais, Hilsenroth, Fowler, and Conboy (1999) found Holt’s measure of PPA to be specifically related to BPD criteria totals compared to HPD, ANPD, and NPD. Findings from this study suggested that PPA was significantly associated with the impulsive and self-destructive behaviors that are common to BPD patients. However, in their follow-up study assessing incremental validity, Blais et al. (2001) did not find PPA to add independently to the prediction of BPD criteria totals.
Gacono et al. (1992) used an early version of the Gacono and Meloy (1994) system and Ag from the CS (Exner, 1986a) to assess the degree of aggression in Rorschach responses in groups of NPD, ANPD, and BPD patients. Although no significant between-group differences were found on these variables, the BPD group produced the most CS Ag responses (mean 1.39) with 72% of the BPD subjects producing at least one Ag response. The NPD group had the next highest Ag totals with a mean of .78 and 50% of the subjects producing at least one Ag response. These authors interpreted their findings as indicating that the “internal world” of BPD patients was “characterized by poorly controlled aggressive and sexual impulses” (Gacono et al., 1992, p. 41).
Westen’s revised SCORS system also contains a measure of aggression called the Experience and Management of Aggressive Impulses subscale (EMAI; see Table 36.4). Ackerman et al. (1999) applied the SCORS to the TAT stories of BPD, NPD, ANPD, and Cluster C PD patients. In this study, BPD subjects obtained significantly lower ratings on the EMAI subscale than did NPD and Cluster C PD subjects, indicating poor control of aggression.
Overall, the findings from the Rorschach and TAT studies reviewed, while not without inconsistencies, support the ability of projective assessment to differentiate BPD subjects based upon both the quality and quantity of aggression present in their profiles (see Table 36.7). As with thought disturbance and defensive function, the assessment of aggression in BPD subjects is aided by applying scales or systems like Holt’s (1977) that were specifically designed to broadly characterize anger and aggression.
BOUNDARY DISTURBANCE AND BORDERLINE PSYCHOPATHOLOGY
Boundary adequacy and stability refers to an individual’s ability to maintain distinctions along cognitive/perceptual and affective dimensions (Fowler, Hilsenroth, & Nolan, 2000). While not specifically reflected in the DSM-IV BPD criteria, boundary difficulties are thought to underlie a number of the BPD behaviors, including unstable affective reactions (BPD Criterion 6), identity difficulties (BPD Criterion 3), and impulsive self-harming behaviors (BPD Criterion 4). Poorly developed (ego) boundaries are prominent features in Kernberg’s model of BPO. The Boundary Disturbance and Thought Disorder Scale (BDS) was developed by Blatt and Ritzler (1974) to rate the degree of both thought disorder and boundary disturbance present in Rorschach responses. With regard to boundary disturbance, the scale measures Boundary Looseness or Laxness (the mildest form of boundary distribution), Inner-Outer boundary disturbance (a midlevel boundary disturbance), and Self-Other boundary disturbance (the most severe form of boundary violation). Several studies using the BDS have shown that borderline patients tend to have more difficulty with Boundary Looseness and Inner-Outer boundary disturbance, while schizophrenic patients have more difficulty maintaining Self-Other boundaries (Blatt & Ritzler, 1974; H.D. Lerner, Sugarman, & Barbour, 1985; Wilson, 1985). Lerner (1991), summarizing these findings concluded: “Thus the findings . . . are consistent in indicating that whereas the development of structural impairment of borderline patients is at the point of inner-outer boundary, for the schizophrenic patient it is at the earlier point of self-other boundary formation” (Lerner, 1991, p. 229). In a recent study comparing self-mutilating (SM) and non-self-mutilating (NSM) BPD patients, Fowler et al. (2000) found that both groups showed problems with boundary integrity. The SM BPD groups produced significantly more signs of severe boundary disturbances (Self-Other) than the NSM BPDs. The finding that SM BPD patients were prone to more serious boundary problems (similar to the boundary problems found in samples of schizophrenic patients) supports the clinical observations that these patients are sicker, more treatment refractory, and difficult to manage (Favazza & Conterio, 1988; Stone, 1987).
ASSESSING THE SEVERITY OF BORDERLINE PSYCHOPATHOLOGY
Both the DSM-IV diagnostic system and Kernberg’s psychodynamic model of personality development allow for a wide range of borderline psychopathology. While all borderline patients can be challenging to treat, clinical experience indicates that some BPD patients are far more challenging then others. Among the most challenging borderline patients are those that engage in self-mutilation. As just reported, Fowler et al. (2000) recently published a Rorschach study comparing SM and NSM BPD patients on a number of theoretically relevant variables. The study is quite informative regarding assessment of severity of borderline psychopathology and the SM variation of BPD. While SM is not by itself a DSM-IV criterion (rather it is one of the behaviors listed under Criterion 5), the presence of this pathological behavior may signal a more severe form of the disorder (Stone, 1987). In their study, Fowler et al. (2000) compared 48 SM BPD patients with 42 NSM BPD patients. All subjects were inpatients at the time of the study. Their findings are informative. The SM BPD group had significantly more primary process aggression (PPA; Holt, 1977); more severely impaired object relations (MOAS; Urist, 1974); used more defensive splitting, devaluing, and idealizing (LDS; P. Lerner & H. Lerner, 1980); and, as reported previously, had more serious boundary disturbance on the BDS than did the NSM group. Clearly, the SM borderline group appeared more pathological on the Rorschach than did the NSM borderline even though both groups were inpatients. These findings hint at the utility of the Rorschach (and possibly other projective instruments), not only for aiding in the classification of patients but also in assessing the severity of their condition.
In addition to its informative findings, this study is worthy of attention because it corrects for many of the methodological shortcomings present in Rorschach research. For example, the study employed an adequate sample size (40# per group) and the two groups were clearly distinguishable (mutilators vs. nonmutilators). The number of planned statistical comparisons was modest (11) and all of the findings were consistent with theoretically based predictions. The methodology of this study provides future researchers with a blueprint that, if followed, would greatly enhance the yield and value of their work. For instance, it would be interesting to explore differences between groups of borderline patients who differ in their tendency to experience brief psychotic, paranoid, or severe dissociative symptoms.
Baity, Hilsenroth, Fowler, Padawer, and Blais (2001) replicated and extended the work of Fowler et al. (2000). In their study, Baity et al (2001) compared 50 BPD patients with 50
nonclinical subjects on psychoanalytic Rorschach scales, including many of those reviewed previously. In addition, their sample of 50 BPD subjects included 35 NSM and 15 SM. The design of the study allows for comparisons among the BPD subjects and nonclinical controls and within the BPD group along the lines of self-mutilation (a marker for severity). The findings were very informative with regard to assessing severity of borderline psychopathology. As would be expected, but until this time not empirically verified, the BPD group scored significantly worse on measures of boundary disturbance (BDS), aggression (PPA and SPA), defensive functioning (LDS), and object relations (MOAS) than did the nonclinical control group. A logistic regression analysis showed that Inner-Outer boundary disturbance, MOAS-PATH (sum of Level 5, 6, and 7 scores) and the defenses of splitting and devaluation predicted BPD diagnosis. Together these four variables accounted for 70% of the variance and correctly classified 93% of the subjects. Within the BPD group the SM BPDs had significantly higher primitive aggression (PPA) and more primitive object relations (MOAS-H) than did the NSM BPDs. While the obtained differences were not as pronounced as in the Fowler et al. (2000) study, these findings show that psychoanalytic scales can differentiate BPD subjects from nonclinical controls and separate the BPD group based on severity (self-mutilating or not).
CONCLUSIONS
“And thus began the search for the Rorschach borderline holy grail: the set of variables, defense configurations, object representations, or object relational patterns that would definitively identify the borderline once and for all. . . . But no borderline holy grail has been found; no definitive Rorschach profile has emerged” (J. Murray, 1993, pp. 342–343).3 Upon completing our review of the empirical and clinical literature, we find ourselves only in partial agreement with Murray’s verdict. It does seem true that no one single projective profile has emerged as being uniquely associated with borderline psychopathology (either BPD or BPO). However, we believe that given the wide range of pathology assumed under both the DSM-IV BPD and Kernberg’s BPO, it is unrealistic to expect a single pattern or collection of test signs to identify (classify) or describe all members of such a heterogeneous group of patients. Furthermore, diagnostic assessment consultation (Blais & Eby, 1998) entails far more than simple sign and pattern recognition. It requires obtaining information from various sources, integrating these data into a relatively comprehensive picture of the patient’s past and current functioning, while also blending into this picture what is currently known (theoretically and empirically) about specific forms of psychopathology and their treatment. The resulting product of this activity should inform patient classification, but also go well beyond this and provide a rich, detailed, and relevant description of the patient’s psychological functioning with clear guidelines for treatment. We believe that the information reviewed previously shows that projective assessment data have sufficient empirical support to be used in pursuing this difficult goal.
There is now an impressive body of research showing that projective data are able to differentiate (not the same as classify) patients with borderline psychopathology from a variety of comparison groups. These comparison groups have included subjects with major depression, schizophrenia, NPD, ANPD, Cluster C PDs, and nonclinical groups. Projective data have been able to identify the unique aspects of borderline psychopathology across a host of theoretically and clinically relevant variables including degree and quality of thought disturbance, level of object relations, nature of defensive functioning, degree and quality of aggression, and boundary stability. The ability of projective assessment to provide such useful and unique information has been greatly advanced by the development of numerous theoretically grounded and psychometrically adequate coding systems.
The findings reviewed suggest that while borderline patients might be wide ranging in how they present on projective assessment, their profiles are typically marked by a number of identifiable features: (1) A mild, but clearly apparent, degree of thought disturbance is usually evident in their record. Indications of this will be most prominent on the Rorschach, but may also be evident in TAT stories, particularly in the patient’s explanations of social causality and possibly in the verbal responses to the WAIS. However, signs of severe thought disturbance, such as multiple CS Level 2 Special Scores or an elevated X– percentage (Exner, 1993) should not be prominent. (2) There should be considerable evidence of primitive, malevolent, and negatively toned object relations. Indications of these negative object relations will be most evident in TAT stories but will also be “visible” in Rorschach responses, particularly responses containing human or animal interactions, and in the recalling of early memories. (3) While somewhat inconsistent, the borderline patient’s Rorschach should contain signs of midlevel defensive functioning. Specifically, the use of devaluation should be prominent in the record, while splitting and projective identification might also be seen, but to a lesser degree. (4) Signs of excessive and primitive aggression should be present in the Rorschach responses, TAT stories, and the patient’s early memories. (5) Lastly, a moderate degree of boundary disturbance, especially signs of Inner-Outer boundary violations, should be evident in the Rorschach material.
Systematically reviewing projective data to determine a patient’s level of functioning across these psychological domains and then organizing these observations into a coherent psychological picture should greatly enhance the clinician’s ability to identify borderline psychopathology and describe aspects of psychological functioning that greatly impact nontest behavior. Approaching projective data in this manner will also allow clinicians to estimate the severity of a patient’s condition and make meaningful predictions regarding treatment.
NOTES
In Rapaport’s system for categorizing thought quality, a fabulized response refers to a response that contains excessive affective elaboration, such as “that’s a mean person.” A fabulized combination denotes a response in which separate details or blot areas are related in an arbitrary or unrealistic manner, such as “it looks like a man attacking submarine.” A confabulized response is one in which a response begins with a small detail and generalizes to a larger area of the inkblot. The initial impression (to the small detail) may be accurate but in total the response is a poor fit to the blot contours: “It’s bird, here’s a beak [good fit to contours] and all of this back here is the bird [poor fit to contours].”
The negative association between BPD total criteria and ROD, a valid measure of implicit dependency needs, reported in Blais, Hilsenroth, Fowler, and Conboy (1999) and Blais, Hilsenroth, et al. (2001) may strike some as unexpected. However, research has shown differences in ROD scores between inpatient and outpatient BPD samples. Bornstein, Hilsenroth, Padawer, and Fowler (2000) explored the range of ROD scores across seven distinct groups including inpatient and outpatient BPD groups. Interestingly, the outpatient BPD group had the lowest ROD scores while the inpatient group had the highest scores. In fact, the difference between the two BPD groups reached statistical significance. While this discrepancy in ROD scores between inpatient and outpatient BPDs awaits replication, it might point to the important and changing nature of dependency in borderline pathology.
The authors want to note that Murray (1993) goes on to describe a sophisticated application of Rorschach data to the understanding of borderline psychopathology that would be quite consistent with many of our views regarding the complexity and utility of assessment consultation activity.
REFERENCES
Ackerman, S.J., Clemence, A.J., Weatherill, R., & Hilsenroth, M.J. (1999). Use of the TAT in the assessment of DSM-IV Cluster B personality disorders. Journal of Personality Assessment, 73, 422–448.
- Acklin, M. (1993). Psychodiagnosis of personality structure II: Borderline personality organization. Journal of Personality Assessment, 61, 329–341.
- American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). Washington, DC: Author.
- American Psychiatric Association. (1986). Diagnostic and statistical manual of mental disorders (3rd ed., revised). Washington, DC: Author.
- American Psychiatric Association. (1994). Diagnostic and statistical manual of mental disorders (4th ed.). Washington, DC: Author.
- Arnow, D., & Harrison, R.H. (1991). Affect in early memories of borderline patients. Journal of Personality Assessment, 56, 75–83.
- Arntz, A., & Veen, G. (2001). Evaluations of others by borderline patients. Journal of Nervous and Mental Disease, 189, 513–521.
- Baity, M.R., & Hilsenroth, M.J. (1999). Rorschach aggression variables: A study of reliability and validity. Journal of Personality Assessment, 72, 93–110.
- Baity, M.R., Hilsenroth, M.J., Fowler, J.C., Padawer, J.R., & Blais, M.A. (2001, March). Primary process aggression and primitive defenses: Self-mutilation and the borderline patient. Paper presented at the midwinter meeting of the Society for Personality Assessment, Philadelphia, PA.
- Baity, M.R., McDaniel, P.S., & Hilsenroth, M.J. (2000). Further exploration of the Rorschach aggressive content (AgC) variable. Journal of Personality Assessment, 74, 231–241.
- Berg, J. (1990). Differentiating ego functions of borderline and narcissistic personalities. Journal of Personality Assessment, 55, 537–548.
- Blais, M.A., Conboy, C., Wilcox, N., & Norman, D. (1996). An empirical study of the DSM-IV Defensive Functioning Scale in personality disordered patients. Comprehensive Psychiatry, 37, 435–440.
- Blais, M.A., & Eby, M. (1998). Jumping into fire: Internship training in personality assessment. In L. Handler & M. Hilsenroth (Eds.), Teaching and learning personality assessment (pp. 485– 500). Hillsdale, NJ: Erlbaum.
- Blais, M.A, Hilsenroth, M.J., & Castlebury, F. (1997). Content validity of the DSM-IV borderline and narcissistic personality disorder criteria sets. Comprehensive Psychiatry, 38, 31–37.
- Blais, M.A., Hilsenroth, M.J., Castlebury, F., Fowler, J.C., & Baity, M.R. (2001). Predicting DSM-IV Cluster B personality disorder criteria from MMPI-2 and Rorschach data: A test of incremental validity. Journal of Personality Assessment, 76, 150–168.
- Blais, M.A., Hilsenroth, M.J., & Fowler, J.C. (1999). Diagnostic efficiency and hierarchical functioning of the DSM-IV borderline personality disorder criteria. Journal of Nervous and Mental Disorders, 187, 167–173.
- Blais, M.A., Hilsenroth, M.J., Fowler, J.C., & Conboy, C.A. (1999). A Rorschach exploration of the DSM-IV borderline personality disorder. Journal of Clinical Psychology, 55, 1–10.
498 Projective Assessment of Borderline Psychopathology
- Blais, M.A., Kelly, J., Holdwick, D., & Hilsenroth, M.J. (2001). The perceived clarity and understandability of the DSM-IV personality disorder criteria sets. Journal of Comprehensive Psychiatry, 42, 466–470.
- Blatt, S., & Ritzler, B. (1974). Thought disorder and boundary disturbance in psychosis. Journal of Consulting and Clinical Psychology, 42, 370–381.
- Bornstein, R.F., Hilsenroth, M.J., Padawer, J.R., & Fowler, J.C. (2000). Interpersonal dependency and personality pathology: Variations in Rorschach Oral Dependency scores across Axis II diagnoses. Journal of Personality Assessment, 75, 478–491.
- Butcher, J.N., Dahlstrom, W.G., Graham, J.R., Tellegen, A., & Kaemmer, B. (1989). MMPI-2: Minnesota Multiphasic Personality Inventory: Manual for administration and scoring. Minneapolis: University of Minnesota Press.
- Colligan, R., Morey, L., & Offord, K. (1994). The MMPI/MMPI-2 personality disorder scales: Contemporary norms for adults and adolescents. Journal of Clinical Psychology, 50, 168–200.
- Cooper, S.H., Perry, J.C., & Arnow, D. (1988). An empirical approach to the study of defense mechanisms: Reliability and preliminary validity of the Rorschach defense scales. Journal of Personality Assessment, 52, 187–203.
- Cramer, P. (1999). Future directions for the Thematic Apperception Test. Journal of Personality Assessment, 72, 74–92.
- Exner, J.E. (1978). The Rorschach: A comprehensive system: Volume 2. Interpretations. New York: Wiley.
- Exner, J.E. (1986a). The Rorschach: A comprehensive system: Volume 1. Basic foundations (2nd ed.). New York: Wiley.
- Exner, J.E. (1986b). Some Rorschach data comparing schizophrenics with borderline and schizotypal personality disorders. Journal of Personality Assessment, 50, 455–471.
- Exner, J.E. (1993). The Rorschach: A comprehensive system: Volume 1. Basic foundations (3rd ed.). New York: Wiley.
- Favazza, A.R., & Conterio, K. (1988). The plight of chronic selfmutilators. Community Mental Health Journal, 24, 22–30.
- Fowler, J.C., Hilsenroth, M.J., & Nolan, E. (2000). Exploring the inner world of self-mutilating borderline patients: A Rorschach investigation. Bulletin of the Menninger Clinic, 64, 365–385.
- Gacono, C.B., & Meloy, J.R. (1994). The Rorschach assessment of aggressive and psychopathic personalities. Hillsdale, NJ: Erlbaum.
- Gacono, C.B., Meloy, J.R., & Berg, J.L. (1992). Object relations, defensive operations, and affect states in narcissistic, borderline, and antisocial personality disorder. Journal of Personality Assessment, 59, 32–49.
- Gartner, J., Hurt, S.W., & Gartner, A. (1989). Psychological test signs of borderline personality disorder: A review of the empirical literature. Journal of Personality Assessment, 53, 423–441.
- Gunderson, J.G. (2001). Borderline personality disorder: A clinical guide. Washington, DC: American Psychiatric Publishing.
- Harris, D. (1993). The prevalence of thought disorder in personalitydisordered outpatients. Journal of Personality Assessment, 61, 112–120.
- Hilsenroth, M.J., Fowler, J.C., & Padawer, J.R. (1998). The Rorschach Schizophrenia Index (SCZI): An examination of reliability, validity, and diagnostic efficiency. Journal of Personality Assessment, 70, 514–534.
- Hilsenroth, M.J., Hibbard, S.R., Nash, M.R., & Handler, L. (1993). A Rorschach study of narcissism, defense, and aggression in borderline, narcissistic, and Cluster C personality disorders. Journal of Personality Assessment, 60, 346–361.
- Holdwick, D., Hilsenroth, M.J., Castlebury, F., and Blais, M.A. (1998). Identifying the unique and common characteristics among the DSM-IV antisocial, borderline and narcissistic personality disorders. Comprehensive Psychiatry, 39, 277–286.
- Holt, R. (1977). A method for assessing primary process manifestations and their control in Rorschach responses. In M. Rickers-Ovsiankina (Ed.), Rorschach psychology (2nd ed., pp. 263–315). Huntington, NY: Krieger.
- Hurt, S.W., Reznikoff, M., & Clarkin J.F. (1991). Psychological assessment, psychiatric diagnosis & treatment planning, New York: Brunner/Mazel.
- Johnston, M., & Holzman, P.S. (1979). Assessing schizophrenic thinking. San Francisco: Jossey-Bass.
- Kernberg, O. (1970). A psychoanalytic classification of character pathology. Journal of the American Psychoanalytic Association, 18, 800–822.
- Kernberg, O. (1975). Borderline conditions and pathological narcissism. New York: Jason Aronson.
- Kircher, T.T.J., Liddle, F.P., Brammer, M.J., Williams, S.C.R., Murray, R.M., & McGuire, P.K. (2001). Neural correlates of formal thought disorder in schizophrenia. Archives of General Psychiatry, 58, 769–774.
- Kleiger, J.H. (1999). Disordered thinking and the Rorschach. Hillsdale, NJ: Analytic Press.
- Knight, R.P. (1953). Borderline states. Bulletin of the Menninger Clinic, 17, 1–12.
- Lerner, H.D., Sugarman, A., & Barbour, C.G. (1985). Patterns of ego boundary disturbance in neurotic, borderline, and schizophrenic patients. Psychoanalytic Psychology, 2, 47–66.
- Lerner, P. (1991). Psychoanalytic theory and the Rorschach. Hillsdale, NJ: Analytic Press.
- Lerner, P., & Lerner, H. (1980). Rorschach assessment of primitive defense in borderline personality structure. In J. Kwawer, H. Lerner, P. Lerner, & A. Sugarman (Eds.), Borderline phenomena and the Rorschach test (pp. 257–274). New York: International Universities Press.
- Lewis, S.J., & Harder, D.W. (1991). A comparison of four measures to diagnose DSM-III-R borderline personality disorder in outpatients. Journal of Nervous and Mental Disease, 179, 329–337.
- Masling, J., Rabie, L., & Blondheim, S. (1967). Obesity, level of aspiration, and Rorschach and TAT measures of oral dependence. Journal of Consulting Psychology, 31, 233–239.
- Mayman, M. (1968). Early memories and character structure. Journal of Projective Techniques and Personality Assessment, 32, 303–316.
- Murray, H.A. (1943). Manual for the Thematic Apperception Test. Cambridge, MA: Harvard University Press.
- Murray, J. (1993). The Rorschach search for the borderline holy grail: An examination of personality structure, personality style, and situation. Journal of Personality Assessment, 61, 342–357.
- Nigg, J.T., Lohr, N.E., Westen, D., Gold, L.J., & Silk, K.R. (1992). Malevolent object representations in borderline personality disorder and major depression. Journal of Abnormal Psychology, 101, 61–67.
- O’Connell, M., Cooper, S., Perry, J.C., and Hoke, L. (1989). The relationship between thought disorder and psychotic symptoms in borderline personality disorder. Journal of Nervous and Mental Disease, 177, 273–278.
- Patrick, J., & Wolfe, B. (1983). Rorschach presentation of borderline personality disorder: Primary process manifestations. Journal of Clinical Psychology, 39, 442–447.
- Rapaport, D., Gill, M., & Schafer, R. (1968). Diagnostic psychological testing (Rev. ed.; R.R. Holt, Ed.). New York: International Universities Press.
- Rorschach, H. (1942). Psychodiagnostics. Bern, Switzerland: Hans Huber. (Original work published 1921)
- Singer, M.T., & Larson, D.G. (1981). Borderline personality and the Rorschach test. Archives of General Psychiatry, 38, 693–698.
- Skelton, M.D., Boik, R.J., & Madero, J.N. (1995). Thought disorder on the WAIS-R relative to the Rorschach: Assessing identitydisordered adolescents. Journal of Personality Assessment, 65, 533–549.
- Steiner, M., Martin, S., Wallace, J., & Goldman, S. (1984). Distinguishing subtypes within the borderline domain: A combined
psychoneuroendocrine approach. Biological Psychiatry, 19, 907–911.
- Stone, M.H. (1987). A psychodynamic approach: Some thoughts on the dynamics and therapy of self-mutilating borderline patients. Journal of Personality Disorders, 1, 347–349.
- Urist, J. (1977). The Rorschach test and the assessment of object relations. Journal of Personality Assessment, 41, 3–9.
- Wechsler, D. (1981). Wechsler Adult Intelligence Scale-Revised. New York: Psychological Corporation.
- Weiner, I.B. (1996). Some observations on the validity of the Rorschach Inkblot Method. Psychological Assessment, 8, 206– 213.
- Westen, D. (1990). Towards a revised theory of borderline object relations: Contributions of empirical research. International Journal of Psychoanalysis, 71, 661–693.
- Westen, D. (1991). Clinical assessment of object relations using the TAT. Journal of Personality Assessment, 56, 56–74.
- Westen, D., Lohr, N., Silk, K.R., Gold, L., & Kerber, K. (1990). Object relations and social cognition in borderlines, major depressives, and normals: A Thematic Apperception Test analysis. Psychological Assessment, 2, 355–364.
- Westen, D., Lohr, N., Silk, K., Kerber, K., & Goodrich, S. (1985). Measuring object relations and social cognition using the TAT: Scoring manual. Unpublished manuscript, University of Michigan, Ann Arbor.
- Westen, D., Ludolph, P., Lerner, H., Ruffins, S., & Wiss, F.C. (1990). Object relations in borderline adolescents. Journal of American Academy of Child and Adolescent Psychiatry, 29, 338–348.
- Widiger, T.A. (1982). Psychological tests and the borderline diagnosis. Journal of Personality Assessment, 46, 227–238.
- Wilson, A. (1985). Boundary disturbance in borderline and psychotic states. Journal of Personality Assessment, 49, 346–355.
- Wood, J.M., Lilienfeld, S.O., Garb, H.N., & Nezworski, M.T. (2000). The Rorschach test in clinical diagnosis: A critical review, with a backward look at Garfield (1947). Journal of Clinical Psychology, 56, 395–430.
Projective Assessment of Psychological Trauma
JUDITH ARMSTRONG AND NANCY KASER-BOYD
INTRODUCTION 500 Theoretical and Clinical Perspectives on Trauma 500 Implications for Projective Test Research 503 RESEARCH FINDINGS 504 Rorschach Trauma Studies—Adults 504
Rorschach Trauma Studies—Children and Adolescents 507 UTILITY OF PROJECTIVE TESTING FOR TRAUMA DISORDERS 509 REFERENCES 510
INTRODUCTION
Psychological trauma is such a profoundly destabilizing phenomenon that one would think it unlikely to mistake, overdiagnose, or entirely miss. Yet trauma disorders take such varied, puzzling forms and their symptoms so mimic and overlap other disorders that they present formidable diagnostic and treatment challenges. To help assessors develop a searching strategy for trauma, we begin with an overview of trauma theory and discuss its implications for projective assessment.
Theoretical and Clinical Perspectives on Trauma
There are two circumstances under which traumatized people come to the attention of assessment psychologists. Some people seek treatment following an identified trauma such as a natural disaster, rape, or life-threatening illness or injury. In these instances the existence and significance of the trauma is overt. Thus, the psychologist will have been alerted to the importance of considering the test data from a trauma standpoint. The contribution of projective tests to understanding what we will call overt trauma presentations has been explored in some detail by assessment researchers (Briere, 1997; Carlson, 1997). Basically, projectives can be helpful in clarifying the myriad clinical issues that are often raised by trauma. As will be discussed in this chapter, post-traumatic stress disorder (PTSD) is only one of many possible trauma outcomes (van der Kolk & McFarlane, 1996). Moreover, PTSD, itself, tends to be associated with multiple comorbidities (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995). The ability of projective tests to illuminate aspects of the patient’s self-concept, affect regulation, relational capacities, and coping mechanisms makes these measures useful in addressing the complexities of trauma diagnosis and treatment (Parson, 1998). For example, projectives can offer important information on whether the patient has the psychological resources to tolerate the stress of the first line of treatment for PTSD, exposure therapy (Foa, Keane, & Friedman, 2000).
Assessment psychologists are also likely to encounter traumatized people under circumstances that are even more diagnostically challenging. This is when trauma reactions are present but are not identified as such. In cases of what we will call covert trauma, patients may be aware of having had an experience, or experiences, that we would label traumatic. However, they are unaware of the connection between such incidents and their present symptoms. Thus, they are unlikely to have brought up these experiences in treatment. A covert trauma presentation is especially likely in cases of chronic childhood abuse and neglect, where traumatic dissociation limits purposeful access to trauma memories (Williams, 1994). However, covert trauma can be found in any patient simply because, by their very nature, traumatic experiences are difficult to capture in words, organize in a coherent fashion, and report in a manner that feels safe (Dalenberg, 2000). Projective tests may give the first sign of the existence of covert trauma since they are particularly useful for gathering data on issues not readily available to self-reflection and selfsharing.
Studies of the prevalence of trauma in psychiatric patients show rates of trauma exposure that range from 60% to over 80% (Bryer, Nelson, Miller, & Kroll, 1987). Reviewing the epidemiological data on traumatic stress, Carlson (1997) concludes that clinicians can expect at least 15% of their adult clients to have current or past trauma symptoms. In view of the ubiquity of trauma in the clinical population and the possibility that the psychological effects of trauma will be complex and covert, it is especially important that assessment psychologists utilize a range of test methods to increase their chances of sampling and recognizing trauma reactions. This means familiarizing themselves with the trauma research literature on projective tests.
The Clinical Faces of Trauma
While the term trauma is used loosely in everyday speech to signify highly unpleasant events, we use the term here in the precise manner described by the Diagnostic and Statistical Manual of Mental Disorders (text revision [DSM-IV-TR]; American Psychiatric Association, 2000). Criterion A-1 for PTSD outlines that a psychological trauma consists of experiencing or witnessing an event that involves death or serious injury to oneself, or learning about the unexpected or violent death of a loved one. Simply undergoing such an experience is not enough. As delineated in Criterion A-2, the person must also react to the experience with intense fear, helplessness, or horror, or if a child, with disorganized or agitated behavior. Thus, being involved in a large-scale disaster as a victim or an emergency worker, being raped, or being tortured would qualify as a Criterion A experience. Being in a minor accident or an emotionally painful relationship or suddenly and unjustly losing a job would not ordinarily meet Criterion A requirements, no matter how personally distressing these experiences are to the individual. The distinction between a traumatic and a noxious experience is important because trauma initiates a set of distinctive psychophysiological responses that are different from the psychophysiology of stress. For example, PTSD patients show a highly sensitized hypothalamic-pituitary-adrenal axis reflecting basic changes in management of arousal level (Yehuda & McFarlane, 1995). Brain norepinephrine system alterations associated with memory and learning disturbance have also been found (Bremner, Davis, Southwick, Krystal, & Charney, 1994). Such physiological reactions underlie the biphasic psychological response to trauma, in which hyperarousal and emotional flooding alternate with avoidance and emotional numbing (van der Kolk, 1994). Physiological dysregulation also underlies the pervasive symptoms that characterize chronic trauma and that can mask accurate diagnosis because they resemble many other psychological disorders.
Common trauma symptoms include somatization, panic reactions, emotional lability, anxiety, agitation, depression, hopelessness, loss of life purpose, sleep problems, inability to self-soothe, and disturbances in thinking and reality testing. Affective disregulation can interact with cognitive confusion and avoidance, producing unbidden, intrusive reminders that plunge the person back into the time of trauma or bleed into ongoing experience. These intrusions can be experienced on a cognitive level as hallucinatory flashbacks, on a somatic level as body pains, and on an emotional level as spurts of grief, fear, or depression (van der Kolk, 1994). Psychoticlike thinking has been observed in traumatized people who were previously clinically normal (Weisath, 1989), and cognitive decline and neurological soft signs have been found in people with chronic trauma (Gurvitz et al., 2000). Traumatic dissociation can cause problems in memory and abrupt alterations in state of awareness that impede the integration of the trauma, making it difficult for the person to talk about the event. Other defensive efforts to avoid being flooded by traumatic memories may make traumatized people appear depleted, uncooperative, and unwilling to engage with the world, further complicating clinicians’ efforts to understand and connect with them.
Not all trauma survivors show these symptoms. There is no one-to-one relationship between an external trauma and the person’s psychological response. Researchers estimate that only 25 to 30% of those exposed to trauma develop PTSD (Green, 1994). Elevated rates of major depression, panic and substance abuse disorders are also commonly observed (Shalev et al., 1998). However, many people spontaneously resolve the trauma and, in the process, develop greater coping skills (Solomon, Mikulincer, & Avitzur, 1988). While such individual variability may be a testament to the uniqueness of the human spirit, it also complicates the researcher’s task.
The Neurobiology of Trauma
As in other psychiatric or psychological disorders, biology or neurobiology is implicated as a cause of clinical symptoms. Emerging data on post-traumatic stress disorder also suggests underlying neurobiological factors in the expression of clinical symptoms. Van der Kolk (1987) asserts that physiological changes can account for most of the post-trauma symptoms noted above. Reviewing studies of inescapable shock and maternal deprivation, he postulated a depletion of a variety of essential neurotransmitters. Kolb (1988), employing classical neurobiological theory, suggested that the experience of massive threat subjects the organism to excessive neuronal overload. Subsequent research supported this hypothesis, finding
a change both in brain chemistry and in brain structure in traumatized subjects.
What sets acute trauma disorders apart from other psychiatric and psychological disorders is the sudden, intense experience of fear (e.g., in traumas like rape, civilian catastrophe, or the experience of criminal assault) or the chronic experience of fear (e.g., in battering relationships or repeated child sexual abuse). Fear or, more precisely, arousal from fear, is controlled by the amygdala, which controls other emotions as well. When the amygdala has been surgically removed in experimental animals, they fail to condition to a feared object (Schachter, 1996). When the amygdala is electrically stimulated in experimental animals, they show a fear response in the absence of a frightening stimulus, and electrical stimulation of the amygdala in patients with temporal lobe epilepsy produces an intense experience of fear (Schacter, 1996). Vietnam combat veterans brain scanned while in a condition that caused intrusive recollections showed heightened activity in the right amygdala and in the visual cortex (Rauch et al., 1996). The amygdala receives input from primary sensory areas of the brain, so that it can receive an “early warning” of danger, and it also receives input from higher cortical structures, where the fear stimuli are further processed.
In most mammals, the experience of fear causes brain changes that help the organism to respond. Adrenaline is released and floods the central nervous system, leading to a chain reaction which includes: (1) changes in the noradrenergic system and in the chemical messengers known as the catecholamines (epinephrine, norepinephrine, and dopamine); and (2) changes in the hypothalamic-pituitary-adrenal axis, with a release of corticotropin-releasing factor (CRF) and then a release of glucocorticoids (cortisol). Epinephrine is associated with arousal states. When rats are experimentally injected with epinephrine they show a fear response (Schacter, 1996) and when human subjects are injected with yohimbine, a drug that mimics arousal states, they also show a fear response. A study with Vietnam veterans revealed an association between the intrusive symptoms of PTSD and the presence of norepinephrine and dopamine in the urine (Yehuda, Southwick, Giller, Ma, & Mason, 1992). Inescapable stress or trauma depletes norepinephrine and dopamine, presumably because use exceeds synthesis; chronic depletion of norepinephrine then renders norepinephrine receptors hypersensitive to subsequent norepinephrine stimulation (van der Kolk & Greenberg, 1987).
During highly stressful experiences, the glucocorticoids (cortisol) are also released in the brain. The glucocorticoids help to mobilize energy for “fight or flight,” increase cardiovascular activity, and inhibit other physiological processes (Schachter, 1996). Flooding with glucocorticoids can seriously damage neurons. Injecting glucocorticoids in rats for several months produces a permanent loss of glucocorticoid receptors in the hippocampus and signs of degeneration of neurons were visible after only a few weeks (Sapolsky, 1992). The hippocampus has been demonstrated to control memory (Schachter, 1996). African primates exposed to various stressors—attacks from other primates, difficulty hiding, and so forth—show abnormally elevated levels of glucocorticoids (Sapolsky, 1992) and atrophy of neurons in the hippocampus. Studies in rats and other experimentally traumatized animals show decreased hippocampal volume (Holschneider, 2000).
Studies with traumatized children and adults show changes in brain structure and chemistry. Neuroimaging of adults and children with PTSD shows a reduction in hippocampal volume, and in children, smaller intracranial and intracerebral volumes (Bremner, 1999; De Bellis et al., 1999). Gurvitz et al. (1996) found a strong positive correlation between degree of Vietnam combat exposure and hippocampal volume. De Bellis, Lefter, Trickett, and Putnam (1994), using magnetic resonance imaging, found a smaller left hippocampus, compared to controls, in women who had suffered severe sexual and physical abuse. Traumatized adults and children also have been found to have adrenergic systems that are more active than normals (Southwick et al., 1990), dysregulated HPA systems (Yehuda & McFarlane, 1995), and abnormalities in serotonergic mechanisms (Southwick et al., 1999).
How might these brain changes tie to specific symptoms of trauma? The negative symptoms of PTSD (e.g., numbing, withdrawal, emotional constriction) are similar to those shown by animals subjected to inescapable shock and may result from the depletion of norepinephrine (van der Kolk and Greenberg, 1987). Reexperiencing traumatic memories in response to a trigger or reminder of the trauma is akin to electrical stimulation of the amygdala, where intense fear reactions in the absence of the original stimulus appear. The biphasic symptoms of PTSD are thought to come from the combination of depletion of norepinephrine and dopamine with the associated hypersensitivity of the neurons to subsequent norepenephrine stimulation (van der Kolk, 1987). In other words, in the absence of a threat stimulus, the individual appears unemotional, flat, or perhaps depressed (like other norepinephrine, and dopamine-depleted patients). A perceived threat causes a surge of epinephrine (like the surge of catecholamines in the original trauma) and this activates the emotions of the original trauma—fear and other emotions. Trauma survivors appear to have a continuing physiological hyperreactivity, which is likely mediated by changes in the noradrenergic system, with noradrenergic receptor hypersensitivity.
Of all of the clinical symptoms, it is the changes in memory that have been the most controversial. Schachter (1996) gives an elegant and easily understood explanation of the underlying brain changes associated with memory deficits. The damage to glucocorticoid receptors in the hypothalamus are likely associated with impaired memory. Experimental animals who have undergone experimental oblation of the hypothalamus but not the amygdala do not appear to avoid a feared stimulus (i.e., have not learned or “remembered” to avoid it) but when it’s presented, they respond with fear. Studies of rats and other animals have shown that injecting epinephrine immediately after an animal learns a task enhances subsequent memory for that task (Schachter, 1996). This helps to explain why trauma-related memories may be unavailable during the constricted phase of the disorder, but the patient is flooded with memories of the trauma when a new threat produces epinephrine.
Dissociation may result from the same biological mechanisms. Dissociated material often surfaces during times of new threat, or when “triggers” or reminders of the trauma occur. This is, again, when epinephrine would be available in the brain. The memories are more inaccessible to the patient with dissociative symptoms, but are likely simply a more extreme end of the spectrum of “forgetting” about or constriction of the memories of trauma. Schachter (1996) points out that dissociation can be horizontal (as in repressing all memories from a part of one’s life) or lateral (forgetting aspects of a portion of one’s life, with otherwise intact memory). Damasio (1989, 1990) hypothesizes that the damage to memory in dissociative patients may stem from damage in the temporal cortex where the information stored “binds” various memories into a coherent “whole.” In dissociative patients, the “binding codes” are lost, impairing memory for specific events.
Research about trauma-induced brain changes is in its infancy, but a discussion of implicated brain changes in PTSD helps explain the myriad changes in cognitive and affective functioning after acute and chronic trauma and lays the groundwork for treatment plans that are truly responsive to the extensive damage that trauma engenders.
Moderating Factors in Trauma
The psychological effects of trauma depend on a variety of moderating factors that influence whether traumatized people will be able to move on with their lives or suffer disabling, long-term psychological effects. It has been increasingly recognized by trauma researchers that trauma reactions cannot simply be conceptualized as an interaction between a normal person and an extraordinary stressor, and
that a diathesis-stress model best reflects the data. Certain variables that influence the trauma response do reside in the external stressor. This includes the magnitude of the trauma, the severity of its violence, and its unpredictability, uncontrollability, and duration (Carlson, Furby, Armstrong, & Schlaes, 1997). Research indicates that highly violent, repetitive trauma has more severe psychological effects than do single or relatively nonviolent incidents (Breslau et al., 1998). Other moderating variables reside within the person. For example, people with an earlier unresolved trauma tend to respond more maladaptively to a new trauma (Resnick, Yehuda, Pitman, & Foy, 1995). Limited coping resources and history of psychological disorder are also predisposing factors for a pathological response to trauma (McFarlane, 1989; Waysman, Schwarzwald, & Solomon, 2001). The developmental stage of the traumatized person is an especially powerful internal moderating variable. Research on repetitive trauma in children indicates that such experiences are likely to have a pervasive effect on personality development (Cassidy & Mohr, 2001). For this reason, in our treatment of the test research here, we will discuss the findings for child and adult populations separately. Still other moderating variables reflect the interaction between the person and the trauma. Involvement in a traumatic situation caused by another person is more likely to lead to a serious psychological reaction than is experiencing an impersonal trauma such as a natural disaster (Briere, 1997). If, as in incest, the relationship between the traumatizer and the traumatized person is close and dependent, it is more likely to lead to a pervasive trauma disorder (Trickett & Putnam, 1993).
At any age, the quality of a person’s social support system functions as a significant protective or risk factor. Positive social support is associated with integration of the traumatic event and subsequent recovery. Conversely, such factors as neglect, family and social disorganization, and simply not talking about a traumatic event with a sympathetic listener predict chronic reactions to trauma (Briere, 1997).
Implications for Projective Test Research
As the previous discussion details, trauma can impact a wide variety of personality and biological functions. Projective test researchers have worked to map the effects of trauma on reality testing, emotional control, object relations, and the process by which neutral stimuli become transformed into traumatic triggers. The sophistication of projective test research has grown with the increasing sophistication of the trauma field. Like the early clinical research, early projective test research did not control for moderating variables such as severity of the traumatic stressor, prior trauma history, and
developmental level of the person at time of trauma. Even now, researchers may not take into account comorbid disorders such as substance abuse, depression, suicidality, and Axis II traits, which may represent secondary reactions to untreated trauma rather than being central trauma responses. (Conversely the same can be said for researchers in other clinical areas, who generally do not control for the effects of past trauma on symptomatology and response to treatment.) In addition, there is little research on subtypes of trauma reactions, such as people who show only a limited trauma response and appear “stuck” in the avoidance, flooding, or overarousal states. These limitations apply to all research on trauma, not just projective tests. We outline them here so that the reader will have a sense of the state of the art of the research to be described and the areas of uncertainty and interest for future investigation.
RESEARCH FINDINGS
The theory that traumatized people have distinctive, intense associations to ambiguous visual stimuli has received unanticipated support in the wake of our recent national trauma, the destruction of the World Trade Center towers on September 11, 2001. Immediately following this, news and web site media documented a widespread and hotly argued debate over whether photographs of a smoke cloud rising over one tower depicted the face of God, the devil, bin Laden, a conspiracy on the part of the photographers to dupe the public, or just a cloud (Wells & Maher, 2001). One psychologist opined that in times of stress the human brain looks for figures in ambiguous, visual stimuli. His description of the rationale for projective testing in cases of trauma received support from an unexpected quarter, the president of the International Association of Arson Investigators, who noted that it was not uncommon for people to see unusual images in smoke clouds (Hoffman, 2001). The earliest projective studies of trauma, done over 20 years ago, used the test best described as photographs of smoke clouds, the Rorschach. As will be described later, these findings became central to the newly developing field of post-traumatic stress.
We have outlined the difficulties diagnosing trauma on the basis of clinical symptoms and the same caveats apply to projective tests. In considering the findings discussed the reader should keep in mind that there is no single, unique, unassailable set of trauma markers. This is especially true for projective test findings since the major use of such tests is the delineation of personality characteristics, not diagnosis. One would expect there to be significant variability in test findings because this would follow the very real variation of symptoms seen in trauma presentations. For example, patients who are more flooded should have different Rorschach patterns from those who are more constricted. Testees who have experienced chronic trauma should similarly show a different pattern of TAT responding from those whose previous functioning was normal. As Briere (1997) has pointed out, projective tests can offer as many pitfalls for misdiagnosis of trauma as do structured tests. No projective test interpretive system is free from theoretical assumptions about the meaning of a response and these assumptions can either blind or illuminate what is observed. Unless the assessor is conversant with the trauma literature, many trauma reactions are likely to be misdiagnosed. Given the complexity of differential diagnosis, and in particular, the potential overlap between trauma, personality disorder, and psychotic test responses, it is essential that clinicians be familiar with all three diagnostic entities in order to make accurate differential diagnoses with projective tests.
Rorschach Trauma Studies—Adults
The earliest studies of Rorschach and trauma involved service people in wartime. The first study of the effects of traumatic stress on Rorschach responses stands as a testament to the determination of the researcher and his subjects. In 1965, Shalit administered the Rorschach to 20 servicemen in the Israeli navy while they were in the midst of a severe storm at sea. This study was the first to demonstrate the rise in inanimate movement (m) that has been consistently found in later trauma research. In 1984, using the newly created diagnosis of PTSD, van der Kolk and Ducey (1984) and Salley and Teiling (1984) studied Vietnam combat veterans and became the first researchers to document traumatic intrusions on the Rorschach. Levin and Reis (1996), in their recent review of the state of Rorschach trauma research, point out that these early studies were important to the development of the trauma field because they helped researchers recognize, and establish an understanding of, the biphasic trauma response.
In the discussion that follows, we combine results from studies of military personnel and civilians because studies find equivalent trauma responses for both populations. Readers will note that most Rorschach research uses the Exner scoring system. However, a number of researchers have used non-Exner scores to capture phenomena not otherwise easily tracked. We first organize our discussion in terms of the biphasic trauma response to enable the reader to put some theoretical organization on the variety of findings described.
Signs of Traumatic Avoidance
Traumatic avoidance has been documented by a number of Rorschach researchers. The low Affective Ratio and low Blends found in these studies has been understood to reflect emotional numbing (Kaser-Boyd, 1993a). The low R and high Lambda (Hartman et al., 1990; Swanson, Blount, & Bruno, 1990) can be understood as markers of cognitive avoidance. These scores combine to produce the unusually low EB generally seen in traumatized populations (Levin & Reis, 1996).
The presence of dissociation is associated with some unique Exner scores. Researchers studying dissociative disordered populations have found an unusual number of super introversive subjects, and this finding is in contrast to the extratensive pattern typically seen in nondissociative trauma groups (Armstrong & Loewenstein, 1990; Scroppo, Weinberger, Drob, & Eagle, 1998). FD, a sign of cognitive and emotional distancing, is characteristic of dissociation (Armstrong, 1991). These findings are consistent with developmental theory that posits that dissociation can enable the child to distance overwhelming emotion and escape into an imaginative world that is more gratifying than the real one (Armstrong, 1994; Putnam, 1997). Using a non-Exner system framework, Leavitt and Labott (1996) and Leavitt (2000) developed and researched a dissociative index that includes references to seeing forms through obscuring medium (similar to the Exner FV), exaggerating the distance of objects (similar to Exner FD), and, a unique variable, disorientation, in which stimuli are seen as shifting or rapidly changing. These researchers were able to correlate their scale with scores on the Dissociative Experiences Scale, suggesting that theirs may be a promising approach to tracking dissociation on the Rorschach (Leavitt & Labott, 1997).
Signs of Traumatic Flooding
Traumatic flooding has been noted in the relatively unstructured color responses (CF # C ! FC) and extratensive EB of trauma populations (van der Kolk & Ducey, 1984, 1989). Painful affect is expressed by the predominance of shading responses, particularly Y and V (Levin, 1993; Salley & Teiling, 1984; Scroppo et al., 1998). It is not surprising that all of the aforementioned researchers find a high negative D and Adjusted D in their samples, given the damaging effects of flooding on coping. Traumatic hyperarousal has been documented by researchers in the significant inanimate movement (m) and Hypervigilant Index (HVI), reflecting overarousal and the sense of helplessness in the face of larger forces. The psychological meaning of the significant HVI seen in trauma populations has been recently explored in a study by Levin, Lazrove, and van der Kolk (1999). Their subjects’ significant HVIs changed from positive to negative following successful eye movement desensitization and reprocessing treatment for PTSD. Using SPECT brain scanning, these researchers were able to show that the decrease in HVI was not associated with changes in limbic system overarousal, but was associated with increased frontal lobe function. They hypothesize that through treatment their subjects become better able to differentiate real from imagined threats and, thus, better able to control their arousal level.
While dissociation is generally viewed as an avoidant process, it can also appear in the flooding phase in the form of flashbacks. Studies have sought to track flashbacks through analysis of content. Since the early Rorschach studies of war and civilian populations, researchers have noted the presence of traumatic content (Leifer, Shapiro, Martone, & Kassem, 1991; van der Kolk & Ducey, 1989). Armstrong (1991), working with a dissociative disorder sample, developed a Traumatic Content Index consisting of the sum of the Exner Content (sex, blood, anatomy, morbid, and aggressive) responses, divided by the total number of responses (TC/R). A TC/R of .3 and above was hypothesized to suggest traumatic intrusions. More recently, Kamphuis, Kugeares, and Finn (2000) documented the ability of the TC/R to distinguish between patients with confirmed sexual abuse and those without abuse. Leavitt and Labott (1996) were able to differentiate women with sexual abuse histories from a control group using non-Exner content indicators of sexual abuse including body damage and images of children as victims. In order to track traumatic intrusions in traumatized Persian Gulf War veterans, Hilsenroth (Sloan, Arsenault, Hilsenroth, Harvill, & Handler, 1995) developed a Combat Content (CC) score. The CC includes perceptions of weapons and personalized responses referring to experiences that occurred during their course of military operations. The Sloan et al. research is particularly notable for its cross-validation of the measures of flooding discussed previously. These researchers found the theoretically expected negative correlation between the MMPI-2 PTSD scale, the PK scale, and the Rorschach D and Adjusted D scales, and a positive correlation between the PK scale and their CC scale. As yet, there exists no trauma content scale that can be applied cross-trauma or cross-culturally. Given the range of potential life traumas, this may be an unrealistic goal. Nonetheless, it is clear that intrusions of traumatic associations onto the Rorschach occur in subjects who may not readily volunteer such information in interview. For example, Franchi and Andronikof-Sanglade (1993) studied a group of West African immigrant women in Paris who had had clitoridectomies. Although none of these women complained of being sexually mutilated, images of intact and clitoridectomized organs alongside scores associated with emotional distress emerged as a dominant theme in 40% of their protocols.
Finally, all trauma researchers have found a high incidence of impaired reality testing and thought disorder on the
Rorschach. This includes atypical views of reality (low X#%, high Xu%), illogical combinations of ideas (incongruous combinations [INCOMs] and fabulized combinations [FABCOMS]), and loss of task focus (DR). Carlson and Armstrong (1994) have argued that for traumatized patients ambiguous tests like the Rorschach can cease to be a test and become, instead, a traumatic trigger. Thus, the typical interpretations of the meaning of scores cannot be utilized, since the testee no longer has the appropriate test set. Similarly, in reviewing the Rorschach trauma literature, Levin and Reis (1996) concluded that traumatic themes often supersede otherwise intact reality testing. Considering that the essence of trauma is dealing with a reality that has behaved in a chaotic and illogical fashion, Armstrong (2002) has hypothesized that these scores reflect a “traumatic thought disorder.” In a study that will be further discussed later, Holaday (2000), researching a traumatized child population, suggested that the SCZI be replaced by a Perception and Thinking Index (PTI) to avoid premature closure on diagnostic questions such as that of trauma versus psychosis. The most recent revision of the Exner system, which includes the new PTI, reflects such a change.
Issues of Interpretation: The State of the Science and Art of the Rorschach and Trauma
Given the biphasic nature of the trauma response, it is not unexpected that Rorschach researchers have documented signs of both flooding and constriction in the Rorschach protocols of traumatized samples. Van der Kolk and Ducey (1984, 1989) and Cerney (1990) reported finding two distinct response modes among their subjects; either constriction with no color determinants or flooding with unmodulated color. In more recent studies, Levin (1993), Swanson, Blount, and Bruno (1990), Hartman et al. (1990), Kaser-Boyd (1993b), and Armstrong (1991) noted a biphasic trauma pattern within their subjects’ protocols. This included emotional lability (CF # C ! FC) alongside a low Affective Ratio (Afr # .05). An avoidance-flooding pattern could also be seen in the combination of high Lambda, low R, and low Afr along with significant Traumatic Content Index, isolated C and CF, and PTI. However, the research treatment of biphasic trauma patterns requires a technique not usually seen in Rorschach research, a statistical treatment of score cluster and sequence analysis. Trauma research awaits the development of such methodology, which should be of great use in bridging from research generalities to questions of differential diagnosis.
Another challenging task awaits clinicians and researchers who seek to untangle Rorschach indicators of chronic trauma from Axis II disorders. Readers may have already noted the parallel between the biphasic trauma response and the Rorschach research findings on patients with borderline personality disorder. This parallel is not unexpected since the two groups overlap, there being a large subgroup of borderlines who report childhood abuse. This said, from a practical standpoint it is clinically important to be able to distinguish between the affective and cognitive variability and malevolent perceptions of people with borderline spectrum disorders and the traumatic intrusions and flooding seen in people with PTSD. The treatment needs, strengths, and vulnerabilities of these two populations are quite different. For example, the splitting implied in the malevolent perceptions of borderline testees is associated with problems in therapeutic relatedness that contrast with the relational issues of traumatized patients momentarily overwhelmed by a flashback. While the presence of trauma does not rule out Axis II disorders, it becomes important for researchers to begin to consider such an issue in developing research designs that are applicable to the reallife tasks of clinicians. Several trauma researchers have already begun to do this. The Sloan et al. (1995) study controlled for premorbid psychiatric condition and premorbid PTSD as well as postmorbid absence of psychiatric disability. Thus, these researchers were able to determine that previous pathology could not account for the low X#%, high m, D, and Ambitents seen in their sample, documenting the powerful, negative effects of trauma on previously adequate personality functioning. Working within the area of traumatic dissociation, Scroppo et al. (1998) found that their dissociative disordered group differed significantly from their borderline control sample. They were able to cross-validate the Armstrong and Loewenstein 1990 study showing that dissociative disordered patients can be distinguished from borderline patients by their high Ms, high whole to part human responses, and the presence of FD and texture responses, all of which suggest a greater ability for objective self-evaluation and relatedness. These studies give promise that the thorny issues of differential diagnosis raised by trauma can be clarified with the help of projective assessment research.
Other Projectives with Adults
While there are a number of recent studies with the Thematic Apperception Test and abused children and adolescents, using Westen’s (1991b) Social Cognition and Object Relations Scale (SCORS), this has not yet been widely applied to the evaluation of traumatized adults. The TAT has been used in creative but not systematic ways in a variety of studies that could be characterized as case reports or small samples (Pica, Beere, Lovinger, & Dush, 2001; Romano, Grayston, DeLuca, & Gillis, 1995).
Rorschach Trauma Studies—Children and Adolescents
Children and adolescents are addressed in this chapter, separate from adults, for several reasons. First, trauma may have different effects depending on the developmental level of the recipient. Next, children have less life history and therefore fewer “intervening variables,” and when we test children, we are likely to be making an assessment closer to the trauma than when we assess adults. Children and adolescents suffer a variety of traumatogenic conditions, including physical abuse, sexual abuse, life-threatening illnesses, accidents, and witnessing community violence (e.g., witnessing parent’s murder). The largest body of research with projective tests has occurred with sexually abused children, followed by a series of studies on children who suffered severe burns. Early work on traumatized children suggested that they may perform within normal limits on structured tests but respond to projective tests with stories that reflect their traumatic experience. However, like adults, there is no single projective test pattern. What is clear from the existing literature on traumatized children is that traumatizing conditions can have an impact on cognitive variables (memory, reality testing, judgment, problem solving) as well as emotion (hyperstimulated, vigilant to danger, emotionally overreactive) and representations of self and others. For example, in one of the most comprehensive current studies of deprived and physically and sexually abused children, aged 6 to 11, Fish-Murray, Koby, and van der Kolk (1987) found these children to be fixated at the preoperational level of development. In comparison to controls, they had difficulty with time sequencing and deficits in social judgment, and they were deficient on measures of self-knowledge and impaired in ability to shift roles or show flexible problem solving. On the Thematic Apperception Test, they exhibited an “all or none” response, either delivering a constricted, impoverished record, or “gruesome tales of murder, kidnapping, beating and abandonment.” The authors note that, on the TAT, some of the children “simply lost all coherence and testing had to be terminated.”
The Rorschach is the most commonly used instrument in traumatized children, followed by the Thematic Apperception Test. A variety of other projective methods (Babiker, 1993) have been proposed but not widely used. The Roberts Apperception Test (McArthur & Roberts, 1982) was created as a child version of the Thematic Apperception Test, but a literature search for the last 10 years found only one trauma study with the Roberts, described as an “exploratory study” (Friedrich & Share, 1997).
The Rorschach
As it is in adults, the Rorschach’s structural data and content are useful indices to current symptoms and psychological processes. The Rorschach allows the user to assess the biphasic response to trauma (Is the child flooded with traumatic images or constricted?); to assess reality testing, affective controls, and perceptions of self and others; but perhaps most importantly, to tap content that reflects the feared stimuli or symbolizes the traumatic experience. In one of the earliest papers on the Rorschach and trauma in children, Viglione (1990) in a single case study discussed a child whose Rorschach showed a high number of “derepressed contents” and was positive on indices of schizophreniclike thinking yet was obviously not psychotic. This is now understood as a common response to trauma—reality testing has been forever altered by the terrible knowledge of one’s vulnerability, but the individual is not psychotic.
Indices and scores that are a measure of trauma response in adults are similar in children. Here, they will be organized by Exner interpretive cluster, but the reader should understand that children also show the patterns of constriction and flooding described in adults previously.
Cognitive Variables
A number of studies found impairments in Rorschach scores that measure cognition and problem solving. In Rorschach language, these are variables in the Exner clusters of Information Processing, Cognitive Mediation, and Ideation.
Zivney, Nash, and Hulsey (1988) examined the Rorschach records of 80 girls aged 9 to 16, with histories of sexual abuse, dividing them into two groups by age at beginning of molestation (before age 9, after age 9). They found the most disturbed girls were those who experienced early abuse and report that over half of these subjects manifested disturbed cognition (M–, low X#%, and more DVs and FABCOMs). Leifer et al. (1991) administered the Rorschach to 38 sexually abused girls aged 5 to 16 and 32 age-matched controls. Seventy-three percent of the abused subjects had experienced penile penetration. The sexually abused girls had more disturbed thinking and impaired reality testing (Wsum6 and X–%).
Children who have suffered traumatic burns (N ” 98), compared to controls have significantly poorer perceptual accuracy (X#% more than three standard deviations apart from controls) and an elevated Coping Deficit Index (Holaday & Whittenberg, 1994). One fourth met the criteria for schizophrenia (SCZI), variables that are mostly cognitive, but did not exhibit psychosis. When the burn group was divided by high and low Lambda (constricted vs. flooded), the biphasic pattern was found. There was no difference between groups when the sample was divided by facial scarring or severity of burns. Almost three quarters of the burn group had burns that were over 5 years old, underscoring the long-term effects of this trauma. Holaday reexamined 20 of these patients at a 3-year follow-up (Holaday, 1998) and found that the group as a whole produced more pathological responses at followup. She attributed this to changes between “constrictive to flooded or flooded to constrictive records,” again supporting the biphasic nature of the trauma symptoms.
Affect
Zivney et al. (1988), in their sample of 80 girls who had been sexually molested, found Rorschach scores suggesting more anxiety and helplessness (m and Y), a damaged self (Morbids), and a “preoccupation with themes of primitive supply and transitional relatedness (food and clothes, X-rays, and abstracts).”
Leifer et. al. (1991), in their study with 79 sexually abused African American girls aged 5 to 16, found higher levels of stress relative to adaptive abilities (EA:ES), higher levels of distress with a preponderance of negative affect (higher DEPI, higher SumShading, and higher Elizur Anxiety Score), more primitive, disturbed human relationships (MOS LOS and higher Elizur Hostility Score), more sexual responses, and higher scores on Fischer and Cleveland’s (1968) penetration score.
Holaday and Whittenberg’s (1994) study of 98 child burn patients found them to be positive on DEPI and to experience more helplessness and anxiety. Elevations on DEPI appeared to be pervasive, with 71% of the sample having four or more of the DEPI variables.
Representations of Self and Others
Holaday and Whittenberg (1994) found their group of burned children to have significantly lower Egocentricity Indices, reflecting their impaired sense of self, and to have significantly less Texture, which is associated with comfort with intimacy.
Two Rorschach studies used the Mutuality of Autonomy Scale, which scores responses for level of developed representations of others. Leifer et. al. (1991), comparing Mutuality of Autonomy scores of the sexually abused group with controls, found disturbed perceptions of interpersonal contact but actual social behavior that was within normal limits. Kelly (1995) examined the object relations of 32 male and female children exposed to repeated trauma (child abuse and neglect) and found that boys had more disturbance in object representation than girls. Object relations were marked by malevolent, destructive, and overpowering figures.
Content
The content of the Rorschach records of children is often a window into their trauma experience. Consider, for example, several responses of a 14-year-old boy whose father had been sent to prison for molesting his sister and who was then charged with molesting his other sister. He had undergone years of a chaotic, frightening, and abusive family situation:
|
A crippled guy with some kind of writing
on his chest. |
|
| Card III |
A dead frog with blood all over.
A person looking at a reflection and there
is blood on the wall. |
|
| Card IV |
A dead animal, his skull has been crushed
and there are parts everywhere. It’s
shattered.
A dead chicken. |
|
| Card V |
A lady putting her hands up to a mirror
and her leg has been cut off. |
|
| Card VI |
A dead fish. |
|
| Card VII |
A pig that’s been blown up and the parts
of him are all separated.
Two elephants that got shot and got all
blown up. |
|
It is statistically rare to see this amount of injury to the human or animal percepts of a young person’s Rorschach. This youngster gives evidence of a self that feels profoundly injured and vulnerable but also angry. Does he fear personal annihilation or does he cope with his own vulnerability with fantasies of destruction? Most likely, he copes with his own vulnerability by projecting anger outward in the classic “victim to aggressor” pattern. It was not a surprise that, for sport, he uses his BB gun to shoot birds near his home.
The Thematic Apperception Test
While the TAT has been in use for over 50 years, systematic research to measure the effects of trauma and differentiate trauma groups from other psychiatric groups began in earnest with the creation of more formal scales for evaluating object relations. This body of work is more developed than any TAT investigation of cognitive variables, and this section of the chapter will focus on representations of self and others in traumatized children and adolescents.
In studying the differences between individuals functioning at different levels of maturity of object relations, it became apparent that histories of child abuse and neglect were associated with the perception of others as malevolent, destructive, and frightening. Two object-relations scoring paradigms currently exist. Westen (1991a), drawing on object-relations theory and social cognition theory, proposed the SCORS, which focuses on the representations of self and others (object relations). Fine (1955) proposed the Scoring Scheme for the TAT and Other Verbal Projective Techniques, which scores TAT scores in terms of feelings, outcomes, and interpersonal relationships. Feelings are categorized as positive, negative, or “other.” Outcomes are categorized as favorable, unfavorable, or indeterminate; and each story is summarized by a single outcome based on its conclusion. Of the two scoring systems, the SCORS has been most frequently used to study traumatized populations. Only one study used the Fine scoring system for a traumatized population. Pistole and Ornduff (1994) used Fine’s Scoring Scheme for the TAT and Other Verbal Projective Techniques with 30 sexually abused female children and a clinical group of 30 female children with no documented history of abuse. Sexually abused children had significantly more negative content (negative feelings and outcomes), and they had higher frequencies of sexual content. The authors compared their findings to clinical reports of sexualized behavior, including sexualized play with dolls, excessive or public masturbation, seductive behavior, and ageinappropriate sexual knowledge in sexual abuse survivors.
The SCORS presents a complex way to view object relations in traumatized subjects. Westen proposed four scales, with focus on different dimensions of self- and other representation. Scale CR is Complexity of Representations of People. The development of concepts of self and others involves the gradual process of increasing complexity and integration. Scale AT is Affect-Tone. Mental representations occur within an affective context. The affective coloring of content ranges from malevolent to benevolent. Perceptions of human relationships range from an expectation that they will be healthy and enriching, to the expectation that they will be painful and abusive. Individuals who have been traumatized are described clinically as more likely to expect that human relationships will be exploitative and abusive. Scale CEI is Capacity for Emotional Investment. Individuals who have experienced human relationships as traumatogenic are likely to avoid making close connections and more likely to stay aloof or become avoidant. Scale USC is Understanding Social Causation. This scale measures the extent to which attributions about the causes of people’s actions, thoughts, and feelings are logical and accurate.
Ornduff, Freedenfeld, Kelsey, and Critelli (1994) used the TAT and the SCORS system to examine the object representations of 17 sexually abused girls and a clinical sample of 25 girls with no history of sexual abuse. Mean object-relations scores differed significantly. The authors note that the representations of abused girls were more primitive, more negative, more punitive, and showed an inability to invest in others except for basic need gratification. They also had difficulty making logical attributions about human interaction.
Freedenfeld, Ornduff, & Kelsey (1995) used the TAT and the SCORS system to compare 39 physically abused children to 39 children with no recorded history of abuse. Physical abuse was associated with a malevolent object world, a lower level capacity for emotional investment in relations, and less accurate, complex, and logical attributions of causality in understanding human interaction. Ornduff and Kelsey (1996) used the TAT and the SCORS system to assess the object relations of 17 sexually abused, 15 physically abused, and 15 distressed but nonabused girls, aged 6 to 16. They found significant differences in overall object relations between the abused and nonabused subjects. Scores reflected lower levels of interpersonal functioning and a propensity for more grossly pathological functioning. The sexually and physically abused girls viewed human interaction as hostile and malevolent. The physically abused girls, in addition, tended to approach relationships and social rules from a perspective of selfgratification.
UTILITY OF PROJECTIVE TESTING FOR TRAUMA DISORDERS
Projective testing, particularly the Rorschach and TAT, may have particular utility for the traumatized patient or client because of its unique ability to capture the subjective experience of the trauma. The patient may be able to communicate trauma images in the indirect mode of the testing situation that were avoided in direct interaction with the treatment provider. We are reminded of the sample of women genitally circumcized (Franchi & Andronikof-Sanglade, 1993), whose Rorschachs contained images of mutilated organs though none spoke directly about their circumcisions.
State-of-the-art treatment interventions frequently recommended for patients with post-traumatic stress disorder are behavior therapies, especially flooding and desensitization, and pharmacotherapy. Projective testing offers an easy and graphic measure of the feared, intrusive images. When used in an informed way by a skilled practitioner, considerable additional data with which to plan treatment (e.g., the fragility of the patient, object relations, reality testing, etc.) is available with projective testing. The use of projective testing in other contexts, for example, in forensic settings, has been dealt with elsewhere (e.g., Kaser-Boyd, 1999).
REFERENCES
- American Psychiatric Association. (2000). Diagnostic and statistical manual of mental disorders (text revision). Washington, DC: Author.
- Armstrong, J.G. (1991). The psychological organization of multiple personality disordered patients as revealed in psychological testing. In R.J. Loewenstein (Ed.), Psychiatric clinics of North America, 14, 533–546.
- Armstrong, J.G. (1994). Reflections on multiple personality disorder as a developmentally complex adaptation. Psychoanalytic Study of the Child, 49, 340–364.
- Armstrong, J.G. (2002). Deciphering the broken narrative of trauma: Signs of traumatic dissociation on the Rorschach. Rorschachiana, 25, 11–27.
- Armstrong, J.G., & Loewenstein, R.J. (1990). Characteristics of patients with multiple personality and dissociative disorders on psychological testing. Journal of Nervous and Mental Disease, 178, 445–454.
- Babiker, G. (1993). Projective testing in the evaluation of the effects of sexual abuse in childhood: A review. British Journal of Projective Psychology, 38, 86–106.
- Bremner, J.D. (1999). Alterations in brain structure and function associated with posttraumatic stress disorder. Seminars in Clinical Neuropsychiatry, 4, 249–255.
- Bremner, J.D., Davis, M., Southwick, S.M., Krystal, J.H., & Charney, D.S. (1994). Neurobiology of posttraumatic stress disorder. In R.J. Pynoos (Ed.), Posttraumatic stress disorder: A clinical review (pp. 43–64). Lutherville, MD: Sidran.
- Breslau, N., Kessler, R.C., Chilcoat, H.D., Schultz, I.R., Davis, G.C., & Andreski, P.C. (1998). Trauma and posttraumatic stress disorder in the community. American Journal of Psychiatry, 55, 626–632.
- Briere, J. (1997). Psychological assessment of adult posttraumatic states. Washington, DC: American Psychological Association.
- Bryer, J.B., Nelson, B.A., Miller, J.B., & Kroll, P.A. (1987). Childhood sexual and physical abuse as factors in adult psychiatric illness. American Journal of Psychiatry, 144, 1426–1430.
- Carlson, E.B. (1997). Trauma assessments. New York: Guilford Press.
- Carlson, E.B., & Armstrong, J.G. (1994). The diagnosis and assessment of dissociative disorders. In S.J. Lynn & J.W. Rhue (Eds.), Dissociation: Clinical and theoretical perspectives. (pp. 159–174). New York: Guilford Press.
- Carlson, E.B., Furby, L., Armstrong, J., & Schlaes, J. (1997). A conceptual framework for the long-term psychological effects of traumatic childhood abuse. Child Maltreatment, 2, 272–295.
- Cassidy, J., & Mohr, J.J. (2001). Unsolvable fear, trauma, and psychopathology. Clinical Psychology: Science and Practice, 8, 275–298.
- Cerney, M. (1990). The Rorschach and traumatic loss: Can the presence of traumatic loss be detected from the Rorschach? Journal of Personality Assessment, 55, 781–789.
- Dalenberg, C.J. (2000). Countertransference and the treatment of trauma. Washington, DC: American Psychological Association.
- Damasio, A.R. (1989). Time-locked multiregional retroactivation: A systems-level proposal for the neural substrates of recall and recognition. Cognition, 33, 25–62.
- Damasio, A.R. (1990). Category-related recognition defects as clues to the neural substrates of knowledge. Trends in Neuroscience, 13, 95–98.
- De Bellis, M.D., Keshavan, M.S., Clark, D.B., Casey, B.J., Giedd, J.N., Boring, A.M., et al. (1999). Developmental traumatology; Part K: Biological stress systems. Biological Psychiatry, 45, 1271–1284.
- De Bellis, M.D. Lefter, L., Trickett, P.K., & Putnam, F.W. (1994). Urinary catecholamine excretion in sexually abused girls. Journal of the American Academy of Child and Adolescent Psychiatry, 33, 320–327.
- Fine, R. (1955). Manual for a scoring scheme for verbal projective techniques (TAT, MAPS, stories and the like). Journal of Projective Techniques, 19, 306–309.
- Fischer, S., & Cleveland, S.E. (1968). Body image and personality. New York: Van Nostrand Reinhold.
- Fish-Murray, C.C., Koby, E.V., & van der Kolk, B.A. (1987). Evolving ideas: The effect of abuse on children’s thought. In B.A. van der Kolk (Ed.), Psychological trauma (pp. 89–110). Washington, DC: American Psychiatric Press.
- Foa, E.B., Keane, T.M., & Friedman, M.J. (2000). Guidelines for treatment of PTSD. Journal of Traumatic Stress, 13, 539–588.
- Franchi, V., & Andronikof-Sanglade, H. (1993). Methodological and epistemological issues raised by the use of the Rorschach Comprehensive System in cross cultural research. Rorschachiana, 18, 118–133.
- Freedenfeld, R.N., Ornduff, S.R., & Kelsey, R.M. (1995). Object relations and physical abuse: A TAT analysis. Journal of Personality Assessment, 64, 552–568.
- Friedrich, W.N., & Share, M.C. (1997). The Roberts Apperception Test for Children: An exploratory study of its use with sexually abused children. Journal of Child Sexual Abuse, 6, 83–91.
- Green, B. (1994). Traumatic stress and disaster: Mental health effects and factors influencing adaptation. In F. Liemac & C.C. Madelson (Eds.), International review of psychiatry, 2 (pp. 117– 210). Washington, DC: American Psychiatric Press.
- Gurvitz, T.V., Gilbertson, M.W., Lasko, N.B., Tarlan, A.S., Simeon, D., Macklin, M., et al. (2000). Neurological soft signs in chronic posttraumatic stress disorder. Archives of General Psychiatry, 57, 181–186.
- Gurvitz, T.V., Shenton, M.E., Hokama, H., Ohta, H., Lasko, M.B., Orr, S.P., et al. (1996). Magnetic resonance imaging study of hippocampal volume in chronic, combat-related posttraumatic stress disorder. Biological Psychiatry, 52, 661–666.
- Hartman, W.R., Clark, M.E., Morgan, M.K., Dunn, V.K., Fine, A.D., Perry, G.G., Jr., et al. (1990). Rorschach structure of a hospitalized sample of Vietnam veterans with PTSD. Journal of Personality Assessment, 54, 149–159.
- Hoffman, B. (2001, September 13). What is that image? Retrieved October 2, 2001, from http://Sa.mlive.com/news/index.ssf?/ news/stories/20010913ssatansface.frm.
- Holaday, M. (1998). Rorschach protocols of children and adolescents with severe burns: A follow-up study. Journal of Personality Assessment, 71, 306–321.
- Holaday, M. (2000). Rorschach protocols from children and adolescents diagnosed with posttraumatic stress disorder. Journal of Personality Assessment, 75, 143–157.
- Holaday, M., & Whittenberg, T. (1994). Rorschach responding in children and adolescents who have been severely burned. Journal of Personality Assessment, 62, 269–279.
- Holschneider, D.P. (2000, September). Genotype to phenotype: Challenges and opportunities in mice and men. UCLA School of Medicine, Department of Psychiatry, Grand Rounds.
- Kamphuis, J.H., Kugeares, S.L., & Finn, S.E. (2000). Rorschach correlates of sexual abuse: Trauma content and aggression indices. Journal of Personality Assessment, 75, 212–224.
- Kaser-Boyd, N. (1993a). Post-traumatic stress disorder in children and adults. Western State Law Review, 20, 319–334.
- Kaser-Boyd, N. (1993b). Rorschachs of women who commit homicide. Journal of Personality Assessment, 60, 458–470.
- Kaser-Boyd, N. (1999). Defending the Rorschach in court. Newsletter of the Society for Personality Assessment.
- Kelly, F.D. (1995). The psychological sequelae of chronic, complex trauma in latency age children: Rorschach indices. Unpublished manuscript, Franklin Medical Center, Greenfield, MA.
- Kessler, R.C., Sonnega, A., Bromet, E., Hughes, M., & Nelson, C.B. (1995). Posttraumatic stress disorder in the national comorbidity study. Archives of General Psychiatry, 52, 1048–1060.
- Kolb, L.C. (1988). A critical survey of hypotheses regarding posttraumatic stress in light of recent research findings. Journal of Traumatic Stress, 1, 291–304.
- Leavitt, F. (2000). Texture response patterns associated with sexual trauma of childhood and adult onset: Developmental and recovered memory implications. Child Abuse and Neglect, 4, 251– 257.
- Leavitt, F., & Labott, S.M. (1996). Authenticity of recovered sexual abuse memories: A Rorschach study. Journal of Traumatic Stress, 9, 483–496.
- Leavitt, F., & Labott, S.M. (1997). Criterion-related validity of Rorschach analogues of dissociation. Psychological Assessment, 9, 244–249.
- Leifer, M., Shapiro, J.P., Martone, M.W., & Kassem, L. (1991). Rorschach assessment of psychological functioning in sexually abused girls. Journal of Personality Assessment, 56, 14–28.
- Levin, P. (1993). Assessing PTSD with the Rorschach projective technique. In J. Wilson & B. Raphael (Eds.), The international
handbook of traumatic stress syndromes (pp. 189–200). New York: Plenum Press.
- Levin, P., Lazrove, S., & van der Kolk, B. (1999). What psychological testing and neuroimaging tell us about the treatment of posttraumatic stress disorder by eye movement desensitization and reprocessing. Journal of Anxiety Disorders, 13, 159–172.
- Levin, P., & Reis, B. (1996). Use of the Rorschach in assessing trauma. In J.P. Wilson and T. Keane (Eds.), Assessing psychological trauma and PTSD (pp. 529–543). New York: Guilford Press.
- McArthur, D.S., & Roberts, G.E. (1982). Roberts Apperception Test for Children: Manual. Los Angeles: Western Psychological Services.
- McFarlane, A.C. (1989). The aetiology of posttraumatic morbidity: Predisposing, precipitating and perpetuating factors. British Journal of Psychiatry, 154, 221–228.
- Ornduff, S.R., Freedenfeld, R.N., Kelsey, R.M., & Critelli, J.W. (1994). Object relations of sexually abused female subjects: A TAT analysis. Journal of Personality Assessment, 63, 223–238.
- Ornduff, S.R. & Kelsey, R.M. (1996). Object relations of sexually and physically abused female children: A TAT analysis. Journal of Personality Assessment, 66, 91–105.
- Pica, M., Beere, D., Lovinger, S., & Dush, D. (2001). The responses of dissociative patients on the Thematic Apperception Test. Journal of Clinical Psychology, 57, 847–864.
- Pistole, D.R., & Ornduff, S.R. (1994). TAT assessment of sexually abused girls: An analysis of manifest content. Journal of Personality Assessment, 63, 211–222.
- Parson, E.R. (1998). Traumatic stress personality disorder (TrSpd), Part II. Trauma assessment using the Rorschach and self-report tests. Journal of Contemporary Psychotherapy, 28, 45–68.
- Pica, M., Beere, D., Lovinger, S., & Dush, D. (2001). The responses of dissociative patients on the Thematic Apperception Test. Journal of Clinical Psychology, 57, 848–864.
- Putnam, F.W. (1997). Dissociation in children and adolescents: A developmental perspective. New York: Guilford Press.
- Rauch, S.L., van der Kolk, B.A., Fisler, R.E., Alpert, N.M., Orr, S.P., Savage, C.R., et al. (1996). A symptom provocation study of posttraumatic stress disorder using positron emission tomography and script-driven imagery. Archives of General Psychiatry, 56, 556–578.
- Resnick, H.S., Yehuda, R., Pitman, R.K., & Foy, D.W. (1995). Effect of previous trauma on acute plasma cortisol level following rape. American Journal of Psychiatry, 152, 1675–1677.
- Romano, E, Grayston, A., DeLuca, R., & Gillis, M. (1995). The Thematic Apperception Test as an outcome measure in the treatment of sexual abuse. Journal of Child and Youth Care, 10, 37–50.
- Salley, R., & Teiling, P. (1984). Dissociated rate attacks in a Vietnam veteran: A Rorschach study. Journal of Personality Assessment, 48, 98–104.
512 Projective Assessment of Psychological Trauma
- Sapolsky, R.M. (1992). Stress, the aging brain, and the mechanisms of neuron death. Cambridge: MIT Press.
- Schachter, D.L. (1996). Searching for memory: The brain, the mind, and the past. New York: Basic Books.
- Scroppo, J.C., Weinberger, J.L., Drob, S.L., & Eagle, P. (1998). Identifying dissociative identity disorder: A self-report and projective study. Journal of Abnormal Psychology, 107, 272–284.
- Shalit, B. (1965). Effects of environmental stimulation on the M, FM and m responses in the Rorschach. Journal of Projective Techniques and Personality Assessment, 29, 228–231.
- Shalev, A.Y., Freedman, S., Peri, T., Brandes, D., Sahar, T., Orr, S.P., et al. (1998). Prospective study of posttraumatic stress disorder and depression following trauma. American Journal of Psychiatry, 155, 630–637.
- Sloan, P., Arsenault, L., Hilsenroth, M., Harvill, L., & Handler, L. (1995). Rorschach measures of posttraumatic stress in Persian Gulf War veterans. Journal of Personality Assessment, 64, 397– 414.
- Solomon, Z., Mikulincer, M., & Avitzur, E. (1988). Coping, locus of control, social support, and combat related posttraumatic stress disorder: A prospective study. Journal of Personality and Social Psychology, 55, 279–285.
- Southwick, S.M., Krystal, J.H., & Morgan, A.C. (1993). Abnormal noradrenergic function in post traumatic stress disorder. Archives of General Psychiatry, 50, 266–274.
- Southwick, S.M., Paige, S.R., Morgan, C.A., Bremner, J.D., Krystal, J.H., & Charney, D.S. (1999). Adrenergic and serotonergic abnormalities in PTSD: Catecholamines and serotonin. Seminars in Clinical Neuropsychiatry, 4, 256–266.
- Swanson, G.S., Blount, J., & Bruno, R. (1990). Comprehensive system Rorschach data on Vietnam combat veterans. Journal of Personality Assessment, 54, 160–169.
- Trickett, P.K., & Putnam, F.W. (1993). Impact of child sexual abuse on females. Psychological Science, 4, 81–87.
- van der Kolk, B.A. (1987). Psychological trauma. Washington, DC: American Psychiatric Press.
- van der Kolk, B.A. (1994). The body keeps score: Memory and the evolving psychobiology of posttraumatic stress. Harvard Review of Psychiatry, 1, 235–265.
- van der Kolk, B.A., & Ducey, C. (1984). Clinical implications of the Rorschach in post-traumatic stress disorder. In B.A. van der Kolk (Ed.), Post-traumatic stress disorder: Psychological and
biological sequelae (pp. 29–42). Washington, DC: American Psychiatric Press.
- van der Kolk, B.A., & Ducey, C. (1989). The psychological processing of traumatic experience: Rorschach patterns in PTSD. Journal of Traumatic Stress, 2, 259–263.
- van der Kolk, B.A., & Greenberg, M.S. (1987). The psychobiology of the trauma response: Hyperarousal, constriction, and addiction to traumatic reexposure. In B.A. van der Kolk (Ed.), Psychological trauma (pp. 63–87). Washington, DC: American Psychiatric Press.
- van der Kolk, B.A., & McFarlane, A.C. (1996). The black hole of trauma. In B.A. van der Kolk, A.C. McFarlane, & L. Weisath (Eds.), Traumatic stress (pp. 3–23). New York: Guilford Press.
- Viglione, D. (1990). Severe disturbance or trauma-induced adaptive reaction: A Rorschach child case study. Journal of Personality Assessment, 55, 280–295.
- Waysman, M., Schwarzwald, J., & Solomon, Z. (2001). Hardiness: An examination of its relationship with positive and negative long term changes following trauma. Journal of Traumatic Stress, 14, 531–548.
- Weisath, L. (1989). A study of behavioral responses to an industrial disaster. Acta Psychiatrica Scandinavica, 355(80), 13–71.
- Wells, S., & Maher, J. (2001, September 28). AP photographer stands by his work. Retrieved October 2, 2001, from http:// 9news.com/newsroom/13294.html
- Westen, D. (1991a). Clinical assessment of object relations using the TAT. Journal of Personality Assessment, 56, 56–74.
- Westen, D. (1991b). Social cognition and object relations. Psychological Bulletin, 109, 429–455.
- Williams, L.M. (1994). Recall of childhood trauma: A prospective study of women’s memories of child sexual abuse. Journal of Consulting and Clinical Psychology, 62, 1167–1176.
- Yehuda, R., & McFarlane, A.C. (1995). Conflict between current knowledge about posttraumatic stress disorder and its original conceptual basis. American Journal of Psychiatry, 152, 1705– 1711.
- Yehuda, R., Southwick, S.M., Giller, E.L., Ma, C., & Mason, J.W. (1992). Urinary catecholamine excretion and severity of PTSD symptoms in Vietnam combat veterans. Journal of Nervous and Mental Disease, 180, 321–325.
- Zivney, O.A., Nash, M.R., & Hulsey, T.L. (1988). Sexual abuse in early versus late childhood: Differing patterns of pathology as revealed on the Rorschach. Psychotherapy—Theory, Research, and Practice, 25, 99–106.
Projective Assessment of Suicidal Ideation
DANIEL J. HOLDWICK JR. AND LEAH BRZUSKIEWICZ
THEORETICAL BASIS AND RATIONALE FOR THE PROJECTIVE ASSESSMENT OF SUICIDAL IDEATION AND SUICIDE RISK ASSESSMENT 513 PROJECTIVE TECHNIQUES IN SUICIDE ASSESSMENT 514 Rorschach Inkblot Techniques 514 Thematic Apperception Test (TAT) 517
The assessment, treatment, and management of suicidal patients are perhaps the most challenging and stressful duties of mental health professionals (Jobes, 1995), requiring treating clinicians to deal with the question of whether “this patient, sitting here with me now, [is] about to commit suicide?” (Maltsberger, 1988, p. 47). Suicide risk assessment is complicated by the fact that suicide is a rare phenomenon, accounting for approximately 32,000 or 1.3% of deaths annually, that has multiple risk factors that vary by age, gender, and ethnicity (National Institute of Mental Health [NIMH], 2001). Conservative estimates place suicidal ideation at a rate of 5.6% (10.5 million persons) annually, with 2.7% (2.7 million) persons making suicide plans and 0.7% (700,000 persons) having attempted suicide (Crosby, Cheltenham, & Sacks, 1999). Clinicians facing the daunting task of evaluating suicidal ideation and determining an individual’s risk for suicide are fortunate to have several assessment models (Clark & Fawcett, 1992; Lovett & Maltsberger, 1992; Maltsberger, 1988; Orbach, 1997; Sa´nchez, 2001) and brief suicide scales available (Goldstein, 2000; Range & Knott, 1997; Rothberg & Geer-Williams, 1992). In light of these methods of assessment, what then is the utility of personality assessment in the evaluation of suicide risk (Eyman & Eyman, 1992)? This chapter provides an update and reanalysis of the literature, with the goal of assisting clinicians in understanding the use of projective techniques in suicide assessment.
THEORETICAL BASIS AND RATIONALE FOR THE PROJECTIVE ASSESSMENT OF SUICIDAL IDEATION AND SUICIDE RISK ASSESSMENT
Numerous tests and methods have been described as projective techniques since the formulation of projection by Murray (1938) and L.K. Frank (1939). However, only a few of these methods have been studied for their descriptive value in understanding suicidal ideation, and fewer still for their potential predictive value in suicide risk assessment. A review of this literature shows that projective tests remain in their infancy as techniques for understanding suicidal ideation, and more specifically in their use for predicting suicidal and selfharming behavior. This may, in part, be due to misunderstandings regarding the concept of projection and the use of empirical methods in investigating projective techniques.
Projection has been described as the process of placing one’s own psychological needs, wishes, desires, or other psychological organization onto an ambiguous stimulus field (Murray, 1938), and projective techniques as any method that affords the opportunity for such processes to occur (Frank, 1939). Projective techniques combine the use of materials that are believed to afford the opportunity for the process of projection to occur with coding systems that quantify responses. In this light, the research of projective techniques is the study of instruments that elicit patient information that is transformed into a code and/or rating scale rather than specifically the study of the projective hypothesis. In its most basic form, the empirical study of projective techniques becomes the customary process of investigating the reliability and validity of the data-gathering process and the coding of the gathered data. Viewing projective techniques for gathering samples of behaviors, cognitive processes, and feelings clarifies the issue at hand in this chapter: Are projective techniques useful in understanding suicidal ideation and risk assessment?
Before examining specific projective techniques in suicide assessment, it is worthwhile to briefly summarize the diagnostic, emotional and cognitive correlates, and hypotheses related to suicide. First, numerous studies have found that suicide is more prevalent in persons diagnosed with mental illness, including depression, substance abuse, schizophrenia, panic disorder, post-traumatic stress disorder, and personality disorders (Orbach, 1997; Sa´nchez, 2001). Schneidman (1993, 1996) has suggested that emotional pain is the primary force involved in suicide. Phenomenological states associated with suicide include hopelessness, feelings of failure, shame and guilt, loneliness, and mood lability (Orbach, 1997, Sa´nchez, 2001). Schneidman (1993) summarized the emotional pains, anguish, aching, angst and dread, and other dysphoric affect that underlies most suicides by coining the term psychache.
Self-destructive processes are considered central to the very notion of suicide (Orbach, 1997). These processes include intrapunitive tendencies to turn aggression inward (Litman, 1967), identification and idealization of a deceased person (Maltsberger & Buie, 1989), boundary disturbances (Blatt & Ritzler, 1974), and self-devaluation (Orbach, 1997). Other factors hypothesized to be related to suicide include the suicidal individual having conflicted dependency yearnings, sober and ambivalent attitudes toward death, high selfexpectations, affective overcontrol, and a tendency to erect barriers to supportive and nurturing relationships and to cope with problems in isolation from others (Smith, 1983; Smith & Eyman, 1988). Perfectionism has also been shown to predict suicidal intent (Hewitt, Flett, & Turnbull, 1992), and it has been suggested that extreme perfectionism can lead to failures that result in depression, anxiety, and suicide (Orbach, 1997). Dichotomous thinking, irrational beliefs, problem-solving deficits, cognitive rigidity, impulsivity, acting-out tendencies, negativism, and identity confusion are additional characteristics of suicidal individuals (Orbach, 1997; Sa´nchez, 2001). Being oversensitive and vulnerable to stress and poor coping skills are also characteristics associated with suicidal ideation (Orbach, 1997, Sa´nchez, 2000).
PROJECTIVE TECHNIQUES IN SUICIDE ASSESSMENT
As noted previously, few projective instruments have been studied empirically in the assessment of suicidal ideation or suicide risk assessment. The following review focuses on projective techniques with empirical studies on suicide ideation and suicide risk assessment, as identified using the American Psychological Association PsychINFO database. We identified articles through PsychINFO using the term suicide coupled with specific test names or acronyms (e.g., Rorschach, TAT) or the term projective and through a careful review of citations in articles collected. Based on this selection method, we identified two projective instruments with moderate empirical study regarding their utility in suicide assessment (Rorschach, TAT) and several promising methods that may have application if subsequent research supports their use (Bender Gestalt, the Hand Test, Human Figures, Incomplete Sentences).
Rorschach Inkblot Techniques
Over the years multiple approaches to scoring the Rorschach and methods for evaluating suicide have been proposed, ranging from single-sign approaches to scale-based methods. Previous reviews of the literature have suggested that the method lacks adequate reliability and validity (Lilienfeld, Wood, & Garb, 2001; Wood, Nezworski, & Stejskal, 1996), and that research using the Rorschach in suicide assessment has yielded inconsistent results (Eyman & Eyman, 1992; Farberow, 1974; G. Frank, 1994; Lester, 1970a; Neuringer, 1965, 1974). In a recent review of the Rorschach, Viglione (1999) found the Comprehensive System for the Rorschach has shown overall good temporal reliability and efficacy as a clinical instrument and that it can be effectively used in suicide assessment with adults, particularly when combined with other methods. In the following pages we examine common strategies used to understand suicide with the Rorschach, including single-sign and configural approaches.
Single-Sign Approaches
Several studies were conducted during the 1940s to 1960s that investigated the use of single cards to detect suicide potential. Lindner (1946) indicated that suicide potential may be indicated in morbid responses (decaying, rotting, or damaged objects) to Card IV. However, subsequent studies (Broida, 1954; Hertz, 1948) did not support this hypothesis. Sapolsky (1963) suggested that responses using the lower center portion of Card VII represented a desire to return to the womb, and he found that suicidal patients gave more responses to this area of the card than nonsuicidal patients. Smith (1981) replicated this finding; however, the majority of studies have not supported Sapolsky’s result (Cooper, Bernstein, & Hart, 1965; Cutter, Jorgensen, & Farberow, 1968; Drake & Rusnak, 1966).
The use of color and color shading has been hypothesized to reflect emotional regulation, and therefore may be useful in the evaluation of potentially suicidal patients. Although Hertz (1948) reported fewer color responses in suicidal patients than nonsuicidal patients, other researchers have not replicated this finding (Blatt & Ritzler, 1974; Fisher, 1951). Appellbaum and Holzman (1962) suggested that responses that combined elements of shading in colored areas (colorshading response) reflected sensitivity to emotional experiences that may lead to significant anxiety and feeling overwhelmed by emotional pain. Appellbaum and Holzman found that suicidal patients provided more responses that combined color and shading elements than nonsuicidal patients, and more color-shading responses in patients that had completed suicides versus attempted suicide. In a later study, Appellbaum and Colson (1968) found the presence of a colorshading response correctly classified 88% of suicidal patients; however, 49% of nonsuicidal patients also gave at least one color-shading response. More recently, Rydin, Asberg, Edman, and Schalling (1990) and Fowler, Hilsenroth, and Piers (2001) found that patients who made a serious suicide attempt had more color-shading responses than parasuicidal and nonsuicidal patients. In contrast, several researchers have not found color shading to discriminate between suicidal and nonsuicidal patients (Blatt & Ritzler, 1974; Cutter et al., 1968; Hansell, Lerner, Milden, & Ludolph, 1988; Neuringer, McEvoy, & Schlesinger, 1965; Smith, 1981).
Cross-sectional and transparency responses have been hypothesized to reflect boundary disturbance, identity confusion, and feelings of emptiness and hopelessness (Blatt & Ritzler, 1974). Several studies suggest that cross-sectional and transparency responses (Blatt & Ritzler, 1974; Fowler, Hilsenroth, et al., 2001; Rierdan, Lang, & Eddy, 1978; Smith, 1981) are robust indicators of suicidal activity. In contrast, a few studies have not found transparency responses to be indicative of current or future risk of suicide (Hansell et al., 1988; Kestenbaum & Lynch, 1978). Hansell and colleagues did, however, find that transparency responses were indicative of past suicide attempts, and that these responses were consistent over time for suicidal patients regardless of whether they were experiencing a depressive episode. This latter finding may indicate that this variable reflects a characterological trait of suicidal individuals, such as hopelessness.
Morbid responses have been interpreted as reflecting a view of the self as damaged and suggestive of despair, selfhatred, and hopelessness (Fowler, Hilsenroth, et al., 2001), as well as associated with depression and suicide (Exner, 1993). Research on the hypothesis that suicidal individuals have more morbid responses than nonsuicidal patients has found some support (Arffa, 1982; Exner, 1993; Fowler, Hilsenroth, et al., 2001; Rydin et al., 1990; Silberg & Armstrong, 1992), while other studies have not found higher rates of morbid responses in suicidal patients (Blatt & Ritzler, 1974; Smith, 1981).
Lastly, a few studies (Kendra, 1979; Smith, 1981) have noted that patients that had completed suicide or made serious suicide attempts had more movement responses than nonsuicidal and parasuicidal patients. Smith suggested that this indicated that patients at highest risk for suicide have greater planning capacity. However, these findings contradict reports of fewer human movement responses in suicidal patients (Hertz, 1948, 1949; Rydin, Schalling, & Asberg, 1982) and Fisher’s (1951) null findings regarding movement responses and suicide. Further research exploring movement as a variable having a bimodal distribution in suicidal patients may clarify the apparent contradictions in previous studies.
Though the presence of a single Rorschach sign of suicide may alert clinicians to the potential of suicide, these signs should be used with caution, and the absence of any single sign should not be interpreted as indicative of low suicide risk (Eyman & Eyman, 1992). This review is suggested for use in assisting in consideration of development of new scales and the interpretation of existing measures.
Multisign/Configural Approaches
Suicide is a complex phenomenon that is likely the result of multiple influences including negative emotional and phenomenological states, self-destructive processes, rigid personality traits, and negative cognitive styles (Orbach, 1997). It is not surprising, then, that single-sign approaches that simplify this phenomena have typically resulted in inconsistent findings across studies. In order to increase the clinical efficacy and more closely approximate the complexity of suicidal ideation, configural approaches use multiple signs as indicators of suicide (Kendra, 1979) and apply a cutoff score to differentiate between suicidal and nonsuicidal patients and/ or degree of suicidality present.
Hertz (1948, 1949) posited that suicidal patients would show higher scores on an index of 10 variables that were hypothesized to reflect neurotic structure, active conflict, anxiety, depression, agitation, emotional outbursts, paranoia, resignation, and withdrawal from the world. Hertz (1948) found that these variables differentiated between groups of suicidal and nonsuicidal patients, and that by using a cutoff score of 5 she was able to correctly identify 94% of suicidal patients and misidentify only 22% of nonsuicidal patients. In her replication study, Hertz (1949) found that 84% of suicidal patients were identified. Sakheim (1955) provided some support for the use of the cutoff score of 5; however, Fisher (1951) found that the cutoff score of 5 did not discriminate between suicidal and nonsuicidal schizophrenic patients, and that this cutoff score misclassified 80% of nonsuicidal schizophrenic patients. Eyman and Eyman (1992) noted that the decline in the use of Hertz’s system appears to be related to the time-consuming nature of determining the presence of each variable and the lack of clarity for calculating the variables. Hertz’s system may be more easily used with today’s technology (Eyman & Eyman, 1992), and it may provide useful insights into refinement of scales for some populations of potentially suicidal patients.
In contrast to Hertz’s (1948, 1949) clinically informed development of a suicide index, Martin’s (1951, 1960, as cited in Eyman & Eyman, 1992) 17 signs for assessing suicide were empirically derived. Martin noted that many of the signs used in his configural approach involved color and shading and may reflect suicidal individuals’ heightened emotional arousal and poor affect control. Martin indicated that the presence of seven or more suicide signs was indicative of suicide and found that this cutoff score correctly classified 69% of suicidal patients. Subsequent studies have provided support for Martin’s indices (Cutter et al., 1968; Daston & Sakheim, 1960; Weiner, 1961). However, Neuringer and colleagues (1965) were unable to differentiate between suicidal and nonsuicidal females, and Weiner (1961) found that a cutoff score of 8 was the best cutoff score, yielding correct classifications of 79% for suicidal patients and 60% for nonsuicidal patients.
Although it has been more than two decades since Exner and Wylie (1977) introduced the initial Suicide Constellation Index (S-CON), to date there have been only two published studies (Exner & Wiley, 1977; Fowler, Piers, Hilsenroth, Holdwick, & Padawer, 2001) that specifically examined the clinical utility of this index with adults. Recently, Acklin, McDowell, Verschell, and Chan (2000) examined the reliability of the Rorschach and found the S-CON and its components to have good interrater and intraobserver reliability, and researchers using the Comprehensive System (Exner, 1986, 1993) approach for assessing suicide have reported good interrater agreement and predictive validity (e.g., Arffa, 1982; Fowler, Hilsenroth, et al., 2001; Fowler, Piers, et al., 2001; Silberg & Armstrong, 1992). One study that found little support for the use of the S-CON with adults (Eyman & Eyman, 1987, as cited in Wood et al., 1996) used an alternate administration procedure and therefore its findings are inconclusive in relation to the S-CON.
Exner and Wylie (1977) found that using a cutoff score of 8 of the 11 variables on the original S-CON correctly classified 74% of persons who completed suicide and 45% of suicide attempters within 60 days of evaluation. This cutoff score also correctly identified 88% of depressed nonsuicidal controls, 94% of nonsuicidal psychotic patients, and 100% of normal controls. In the revision process of the scale (Exner, 1986, 1993), the addition of the indicator “morbid response ! 3” improved the correct classification of suicidal patients to nearly 80%. After further refinement, Exner indicated that the S-CON correctly identified 83% of suicidal patients, with acceptable false-positive (10%) and false-negative rates (15%). In a replication and extension of Exner’s work, Fowler, Hilsenroth, and colleagues (2001) found that the S-CON was able to discriminate between suicidal and nonsuicidal patients, as well as between suicidal and parasuicidal patients. However, Fowler, Hilsenroth, and colleagues found that a cutoff score of 7 rather than 8 was best in differentiating between persons making a serious suicide attempt versus nonsuicidal and parasuicidal individuals (81% true-positive rate).
Attempts to develop an adolescent scale for suicide assessment have met with mixed results (Arffa, 1982; Exner, 1993; Silberg & Armstrong, 1992). Arffa examined the use of the 10 signs identified by Exner and Wylie (1977), as well as Lindner’s (1946) and Sapolsky’s (1963) signs, and a composite score of these 12 variables was calculated. Analyses found that suicide attempters scored higher than nonattempters on the overall scale. Using a cutoff score of 4 as indicative of suicide, Arffa found that 92% of suicide attempters were correctly classified and 25% of nonsuicidal individuals were misclassified. Silberg and Armstrong (1992) explored the use of the revised S-CON with adolescents and found that it did not discriminate between suicidal and nonsuicidal groups. Using discriminant analysis, Silberg and Armstrong reported that the presence of vista responses, morbid responses, poor form quality in movement responses, multiple color-shading blends, color plus color form responses exceeding form color responses, and the weighted special score exceeding 9 were useful in distinguishing between suicidal and nonsuicidal adolescents, and that the presence of four or more indicators correctly classified 64% of suicidal patients, and falsely identified 15% of depressed nonsuicidal patients and 25% of patients who were neither suicidal nor depressed. Unfortunately, no additional studies were found that replicated the findings of Arffa (1982) or Silberg and Armstrong (1992).
A final note on the S-CON relates to its use with child and adolescent populations. No participants in the development or validation studies of the S-CON were under age 18 (Exner, 1986; Exner & Wylie, 1977; Fowler, Hilsenroth, et al., 2001), and attempts to develop a child and adolescent version of the S-CON have met with unacceptably high false-positive and false-negative results (Exner, 1993) or have not supported its use (Arffa, 1982; Silberg & Armstrong, 1992). Though Exner suggests that the S-CON not be used with persons under age 15 (based on positive results in an unpublished study of 15- and 16-year-old suicidal patients), we believe that clinicians should not interpret the S-CON with persons outside of the normative sample until published studies supporting its clinical efficacy are available.
An ego-analytic method of analysis has also been applied to the study of suicide with the Rorschach (Rydin et al., 1990; Rydin et al., 1982). Rydin and colleagues (1982) investigated the relationship between 19 psychogram variables using the Rorschach and CSF 5-HIAA, a measure of metabolized serotonin, with depressed and suicidal patients. They found that individuals low in CSF 5-HIAA had fewer inanimate movement responses, fewer human movement responses, and a higher percentage of accurate pure form responses. In addition, Rydin et al. (1982) found that low 5-HIAA patients had (1) higher color to human movement ratios, (2) higher indices for anxiety, hostility, depressive inhibition, and paranoid attitudes, and (3) lower scores on anxiety tolerance, handling of conflict, and global ratings of psychological adjustment. Applying this approach to the study of violent versus nonviolent suicidal patients, Rydin and colleagues (1990) found that violent suicidal patients could be differentiated from nonviolent suicide attempters and nonsuicidal patients on the basis of lower scores on scales of tolerance of dysphoric affect, handling of conflict, reality testing, and developmental level, and higher scores on measures of paranoid attitude, immature cognition, primitive thought, and hostility. Discriminant analysis based on six indices (developmental level, reality testing, handling of conflict, dysphoria tolerance, primitive thought, hostility) correctly classified 63% of patients as violent attempters, nonviolent attempters, or nonsuicidal (Rydin et al., 1990).
Recently, a scale based on a psychoanalytic formulation of suicide was developed using existing Rorschach variables (Fowler, Hilsenroth, et al., 2001). In a sample of emotionally disturbed adult inpatients, Fowler and colleagues investigated the utility of four variables associated with feelings of depression and self-hate (morbid images), boundary disturbance (transparency and cross-sectional responses), and poor affect regulation (Appellbaum’s color-shading blend). Excellent interrater agreement was found for scoring each of the above
response categories. Consistent with previous research, suicidal patients were found to have more morbid, transparency, cross-sectional, and color-shading responses. The Riggs Index, the sum of each instance of the above four variables into a total score, was found to discriminate between suicidal patients and patients who were parasuicidal or nonsuicidal. Diagnostic efficiency statistics calculated for their sample suggested that Riggs Index scores of 5 or greater were found to yield overall correct classification of .80. The Riggs Index appears to be a promising approach to using the Rorschach in suicide assessment, and future studies are encouraged to explore its use with diverse populations, including adolescents and outpatient samples.
Consistent with Eyman and Eyman (1992), the Rorschach appears to be a useful instrument in the assessment of suicide. It is our view that the configural approaches provide the best reliability and discriminant validity. Although the configural approaches developed by Hertz (1948, 1949) and Martin (1951, 1960, as cited in Eyman and Eyman, 1992) appear to be promising, no studies on their use have been published for several decades and they appear to no longer be in use. Exner’s S-CON (1993; Exner & Wylie, 1977) appears to adequately predict suicide in adults; however, it has not been shown to be valid in assessing suicide in children or adolescents. The Riggs Index (Fowler, Hilsenroth, et al., 2001) also shows promise in assessing suicide with emotionally disturbed adults and may be used cautiously in evaluating suicidal ideation. Further research examining the S-CON (Exner, 1993), Riggs Index (Fowler, Hilsenroth, et al., 2001), egoanalytic approach by Rydin and colleagues (1982, 1990), and adolescent scales developed by Arffa (1982) and Silberg and Armstrong (1992) would likely further our understanding of the strengths, limitations, and range of application for these scales. In addition, the Rorschach may be useful within a battery of tests, using the procedure developed by Smith and Eyman (1988), described in the following section on the TAT.
Thematic Apperception Test (TAT)
Previous reviews of the TAT in suicide assessment indicated that little research has been conducted regarding the utility of the TAT in suicide assessment, and that studies using the TAT had failed to differentiate between suicidal and nonsuicidal patients (Bongar, 1991; Eyman & Eyman, 1992). Although Bongar (1991) indicated that the TAT had not adequately been shown to be useful in suicide assessment, Eyman and Eyman (1992) suggested that the TAT can be useful within a battery of tests because it commonly elicits themes of death that reflect attitudes toward death and dying. The TAT may also provide useful information regarding the individual’s interpersonal issues, emotional states, interpersonal coping styles, and situations in which the person may feel overwhelmed (Eyman & Eyman, 1992). In recent years, a number of new methods for scoring the TAT have been developed that have shown good reliability and validity (Cramer, 1999; Westen, 1991), and a new generation of researchers have begun to reexamine the utility of the TAT with suicidal patients (Gutin, 1997; Litinsky, 1997; Ngai, 2001; Vivona, 1997).
Studies using the TAT in suicide assessment have tended to use theme interpretation and clinician judgment to assess for the presence of suicide (Adkins & Parker, 1996; Broida, 1954; Schneidman & Farberow, 1958; Smith, 1981), indicators of aggression (Fisher & Hinds, 1951; Lester, 1970b; Levinson & Neuringer, 1972; McEvoy, 1974), and various combinations of TAT cards. Research to date has found no differences between suicidal and nonsuicidal patients with the TAT in the themes generated to Card 3BM (Broida, 1954), the number of presses mentioned by adolescents in their TAT stories (Levinson & Neuringer, 1972), amount of aggressive content (Fisher & Hinds, 1951; Lester, 1970b; McEvoy, 1974), presence of suicide stories (Smith, 1981), and feelings of hopelessness (Smith, 1981). In addition, researchers using the TAT have found no difference between suicidal and nonsuicidal college students (Adkins & Parker, 1996) or in clinician ratings of suicidality based on review the description of heroes in patient TAT stories (Schneidman & Farberow, 1958).
Other researchers have examined the relationship between TAT stories and life events (Taylor, 1984), its use within a battery of tests (Smith, 1981, 1983; Smith & Eyman, 1988), and with potentially suicidal individuals (Gutin, 1997; Litinsky, 1997; Ngai, 2001; Vivona, 1997). For example, individuals who had lost a parent through death or divorce generated more themes of death and suicide than participants who had not lost a parent during childhood (Taylor, 1984), and suicidal patients have been found to show selected forms of dichotomous thinking as compared to nonsuicidal patients (Litinsky, 1997). Recently, researchers have explored the use of Westen’s (1991) Social Cognition and Object Relations Scale (SCORS) in order to examine the role object relations may have in suicide. Vivona (1997) suggested that object relations play a mediating role between early traumatic experiences and later suicidal behavior, and Gutin (1997) found that borderline patients had more suicide-related themes than narcissistic patients. Contrary to expectation, Ngai (2001) found that suicidal adolescents appeared less disturbed than nonsuicidal adolescents, with nonsuicidal adolescents showing more hostility, malevolent representations, and need gratification orientation than suicidal adolescents.
Smith (1983) and Smith and Eyman (1988) examined the utility of a set of tests, including the TAT and Rorschach, to predict and describe suicidal activity from an ego-analytic view of suicide. In the initial study, Smith (1983), using a qualitative approach, found that blind raters could correctly classify 85% of cases as having completed suicide, having made a serious or mild suicide attempt, and nonattempters. Smith and Eyman (1988) later found that males that had made serious suicide attempts, as compared to mildly suicidal males, tended to show (1) more overcontrol and have more aggressive ideation, (2) higher self-expectations, (3) conflicted dependency and nurturance needs, and (4) more ambivalent feelings toward death. In contrast to Smith’s (1983) earlier study, serious and mildly suicidal patients were found to differ in that seriously suicidal females showed higher rates of overcontrolled emotion. Patients showing three of the four features examined (affective overcontrol, high self-expectations, conflicted dependency needs, ambivalent and serious attitudes toward death) were more likely to belong to the seriously suicidal group (69%) than the mildly suicidal group (27%), and this trend was more pronounced with male patients (85% seriously suicidal, 30% mildly suicidal) than female patients (54% seriously suicidal, 23% mildly suicidal). These works suggest that the TAT may be useful, within a battery of tests, in eliciting personality styles that predispose an individual toward suicidal activity and assist in the prediction of suicidal behavior.
The TAT remains questionable in the assessment of suicide. In large part this is due to the lack of replicated studies and the variation in selected cards and scoring methods used across studies. Some research suggests that it may be useful within a battery of instruments (Smith, 1983; Smith & Eyman, 1988); however, these studies did not examine whether the TAT is necessary or sufficient for exploration of ego structures associated with suicidal patients. More recent doctoral dissertations (Gutin, 1997; Litinsky, 1997; Ngai, 2001) suggest that the TAT may be useful when combined with Westen’s (1991) SCORS approach for evaluating object relations. Further examination of this latter method and Smith and Eyman’s (1988) ego-analytic approach appears to be warranted; however, clinicians are recommended to use the TAT cautiously in evaluating suicidal ideation and risk for self-harm until further studies have been conducted.
Bender Gestalt, Hand Test, Human Figure Drawings, and Incomplete Sentences
In addition to the Rorschach and TAT, several other projective techniques have received limited empirical study for the purpose of evaluating suicidal ideation and estimating risk for self-harm. The following section focuses on potential areas of clinical utility for these instruments and offers suggestions for further research. At present, the state of knowledge for each of these instruments is limited, and it would be prudent to await further research prior to incorporating their use in the assessment of suicide.
Bender Visual-Motor Gestalt Test
Though most commonly used as an instrument for screening neurological impairment (Groth-Marnat, 1990), the Bender Gestalt has seen multiple uses over the years, including projective assessment of personality and the evaluation of suicide (Kenny, Rohn, Sarles, Reynolds, & Heald, 1979; Leonard, 1973; Sternberg & Levine, 1965). Sternberg and Levine found that 88% of patients showing penetration of Design 6 into Design 5 had expressed some degree of suicidal ideation during hospitalization. Subsequent research found that suicidal individuals showed greater difficulty in maintaining Design 2 in a horizontal position (Leonard, 1973) and made significantly more errors when the Canter Background Interference Procedure was used with the Bender Gestalt Test (Kenny et al., 1979). It has, however, been more than two decades since any research on the use of the Bender Gestalt Test for suicide assessment has been published. These studies used a single-sign approach, a method that is likely to limit detection of complex behaviors such as suicide. Future research with the Bender Gestalt would be most useful in limited areas where the test is already in common use; for example, in neuropsychological screenings (Groth-Marnat, 1990). One population at increased risk for suicide is head injury patients (Mann, Waternaux, Haas, & Malone, 1999), and the development of a suicide risk scale for the Bender Gestalt that uses the above determinants and additional signs of emotional distress (see Groth-Marnat, 1990; Leonard, 1973) may be beneficial within neuropsychologically impaired populations.
The Hand Test
Originally developed by Bricklin, Piotrowski, and Wagner (1962) and revised by Wagner (1983), the Hand Test is a brief projective instrument that has been found to be a reliable and valid measure of personality with children, adolescents, and adults (Clemence, Hilsenroth, Sivec, Rasch, & Waehler, 1998; Hilsenroth, Fowler, Sivec, & Waehler, 1994; Sivec & Hilsenroth, 1994; Wagner, 1983). To date, no studies have been published that have examined the Hand Test in evaluating suicidal ideation and self-harm. A glimpse of the possible efficacy of the Hand Test in suicide risk evaluation may be found in Anders’s (1998) dissertation of adult suicidal patients. Anders found suicidal patients to differ from nonsuicidal patients on four scores on the Hand Test (Acting-Out, Aggression, Direction, Communication). The Hand Test’s Acting-Out Ratio and Tension scores were also found to positively correlate with measures of suicidal ideation and hopelessness, respectively, and the Communication score was found to negatively correlate with suicidal ideation. Although clinical use of the Hand Test may assist clinicians’ understanding of patients’ expressed needs and desires regarding suicide, there exists a need to replicate and extend Anders’s findings. In addition, development of a suicide scale using multiple determinants would likely increase reliability and clinical efficacy in comparison to the isolated single signs studied by Anders.
Human Figure Drawings (HFDs)
Reviews of projective drawing techniques have often found that they lack adequate reliability and validity (Groth-Marnat, 1990; Kahill, 1984; Roback, 1968) and that the research literature is bereft with contradictory results (Groth-Marnat, 1990). More recently, researchers have shown increased interest in Human Figure Drawings (McNeish & Naglieri, 1993; Naglieri & Pfeiffer, 1992; Tharinger & Stark, 1990). In relation to suicide assessment, several authors (Machover, 1949; Orbach, 1988; Virshup, 1976) have suggested the use of HFDs in the assessment of suicide in children. Machover (1949) noted that suicide attempters may pay particular attention to the neck area, and Virshup (1976) suggested that loops and slashes indicated a desire to hang oneself.
A multideterminant scale to assess for suicide risk using the HFD was developed by Richman and Pfeffer (Richman, 1972, and Richman & Pfeffer, 1977, as cited in Zalsman et al., 2000). The scale consists of nine categories of indicators associated with suicide: decompensatory defenses, impulse control disorder, organic indicators, psychotic indicators, depression, denial and projection, dissociative signs, overt aggression, and specific indicators of suicide. The overall scale consists of 27 indicators and the clinician’s overall impression. The HFD is administered in the standard manner (see Anastasi, 1988; Groth-Marnat, 1990), then each of the 28 items are rated using a 5-point Likert scale. According to Zalsman and colleagues (2000), Richman and Pfeffer (1977) reported that they could correctly identify 70% of children as suicidal or nonsuicidal. Pfeffer and Richman (1991) reported in later research that the “specific indicators of suicide scale” were the best predictor of suicidal behavior.
Zalsman and colleagues (2000) recently investigated the interrater reliability, internal consistency, and concurrent validity of Richman’s scale. Using discriminant analysis, Zalsman and colleagues found the scale correctly classified 84.6% of suicidal and 76.5% of nonsuicidal adolescent patients, and that seven indicators were found to correlate significantly with severity of suicide as measured by a semistructured interview. Internal consistency and interrater reliability for the nine categories were generally adequate. However, interrater agreement on the “denial and projection” category was low, and the internal consistency for several indices was considered low. Though promising, the HFD remains limited in its use for suicide risk assessment due to the lack of an established scale and/or cutoff scores for interpretation and risk estimation. In addition, internal consistency for the overall scale is unknown at this time. Further refinement of the scale through clarification of the definitions for rating specific items, factor analysis of specific items, and investigation of the relationship between the indicators and related constructs would likely assist clinical interpretation. The promising findings regarding the HFD (Pfeffer & Richman, 1991; Zalsman et al., 2000) suggest that further research using this approach for suicide risk assessment in children and adolescents is warranted.
Incomplete Sentences Blanks (ISBs)
Several different sentence completion tasks and rating methods have been developed and researched in relation to suicide ideation and risk assessment (Browning, 1986; Efron, 1960; Lehnert, Overholser, & Adams, 1996; Rohde, 1957; Rotter, Lah, & Rafferty, 1992; Rotter & Rafferty, 1950). In an early study of the ISB technique, Efron (1960) found that clinical decisions regarding patient suicide solely based on a review of ISBs were not significantly better than chance. It is noted, however, that Efron’s examiners were simply reviewing a set of ISBs without aid of specific dimensions or scoring techniques. Introducing more structure and systematic scoring to ISB methods, Rohde (1957) developed a system in which participant responses were rated for the frequency and intensity of expressed needs. It was suggested interpretation be done based on a review of all responses, rather than single items, and include three levels of analysis: examination of overt content, review of formal aspects of the protocol, and inference of personality dynamics. Though Rohde developed an elaborate scoring system for patients’ overt and latent needs, as revealed through responses to the ISB, including coding of verbal and physical intraaggressive statements hypothesized to be related to suicidal ideation, no systematic data to support these ideas have been published.
The most commonly used ISB, the Rotter Incomplete Sentences Blank (Rotter et al., 1992; Rotter & Rafferty, 1950), introduced a simplified scoring method focusing on the presence or absence of conflict that leads to a single overall rating of maladjustment, with interpretation being largely based on qualitative content analysis and clinical impressions. Using their scoring method, Rotter and Rafferty (1950) and Rotter et al. (1992) found good split-half and interrater reliability, and the overall maladjustment score was found to correlate with clinician ratings and self-report measures of problems and maladjustment. Although the Rotter ISB may yield information regarding patients’ ideas related to suicide, no published studies have specifically investigated its use in identifying suicidal patients and neither manual specifically addresses its use in evaluating suicidal individuals.
In contrast to the largely qualitative methods used by Rohde (1957) and Rotter and colleagues (Rotter et al., 1992; Rotter & Rafferty, 1950), the Cognition Rating Form (CRF) uses a simplified, 15-minute scoring procedure with the Rotter ISB (Lehnert et al., 1996). The CRF consists of 25 categories designed to measure a wide range of cognitive thinking styles associated with negative affect and pathology, as well as positive adjustment and adaptive attitudes. Scoring involves rating each of the incomplete sentences for the presence or absence of 25 types of cognitions, and summary scores are calculated for each category of cognitions. Lehnert and colleagues (1996) indicated that 10 of the CRF’s cognition categories showed good interrater reliability, with 15 categories showing interrater agreement below .70. Subsequent analysis suggested that CRF scales may be useful in discriminating depressed and suicidal adolescents from normal controls and nonsuicidal individuals, respectively. However, the CRF remains a scoring method in development with likely revision in the content of ISB stems, categories rated, and method of rating identified cognitive categories. The CRF method appears to be a promising approach to quantifying ISB responses, and further research with this semistructured technique is encouraged.
SUMMARY AND FUTURE DEVELOPMENTS
We began this chapter with the question of what, if any, role projective techniques might play in evaluating suicidal ideation and patient risk for self-harm. Although projective techniques remain in their infancy regarding empirical evidence for their use in suicide risk assessment, several promising methods may be on the horizon to join the Rorschach in assisting clinicians working with potentially suicidal patients. New research on the Thematic Apperception Test, the Hand Test, and Cognition Rating Form for the Rotter ISB suggests that these techniques may provide useful information regarding characteristics of adult suicidal patients. At this time, only the Human Figure Drawing has shown specific promise in evaluating suicide risk with children. Evaluating suicide risk with adolescent patients, using projective techniques, remains problematic; however, scales for the Rorschach and Hand Test may prove useful if further research replicates earlier findings. The Bender Gestalt may have limited utility in suicide assessment with head injury and related populations, though this technique appears less likely than other projective methods to develop a sufficient database for its use in suicide assessment. The Comprehensive System’s Suicide Constellation (Exner, 1993; Exner & Wylie, 1977; Fowler, Piers et al., 2001) remains the only projective scale replicated as a predictive measure of future suicide. The newly developed Riggs Index (Fowler, Hilsenroth, & Piers, 2001) for the Rorschach may also be used with caution in evaluating for suicidal ideation and risk for self-harm. Further research investigating the reliability (interrater, intraobserver); concurrent, predictive, and discriminate validity; and general clinical utility for suicide assessment remains a necessary endeavor due to our limited state of knowledge regarding projective techniques for the purpose of suicide assessment.
It should be noted that personality tests as a whole may be poorly equipped to determine immanent lethality and specific symptomatic behaviors associated with suicide (Eyman & Eyman, 1992), a view similarly noted in a recent review of objective personality tests (Johnson, Lall, Bongar, & Nordland, 1999). Personality assessment, whether self-report or projective techniques, may be more useful in evaluating psychological characteristics that predispose someone to suicide (Eyman & Eyman, 1992; Smith & Eyman, 1988). Orbach (1997) and Sa´nchez (2001) outlined several dimensions that are useful for clinicians in the assessment of suicidal ideation and patient’s risk for self-harm. In particular, mental and phenomenological states, self-destructive processes, personality traits, and an individual’s perception of his or her personal and environmental stressors may be available to clinicians through personality assessment methods. In addition, projective assessment techniques may be useful in understanding protective factors that buffer individuals from suicidal ideation and pain associated with loss (e.g., experiencing relationships as supportive and nurturing). At present, however, these statements remain largely hypotheses in need of further study. It is recommended that researchers further investigate the relationship between constructs associated with suicide and specific measures and indicators used with projective techniques. In particular, researchers are encouraged to investigate the convergent and incremental validity of projective techniques with self-report and other methods of assessment while being cognizant of factors that can affect validity estimates (Meyer, 1997, 1999; Meyer, Riethmiller, Brooks, Benoit, & Handler, 2000).
Projective techniques may be at a competitive disadvantage in comparison to less time-consuming methods of information gathering (e.g., clinical interview, self-report techniques). However, remembering that the goal of suicide assessment is in gathering information that assists clinicians in making determinations regarding their patients’ proximal and distal risk for self-harm is important. Projective techniques appear most likely to be useful in predicting distal risk for self-harm and in describing motivations and situations when self-harm becomes more likely. Projective techniques may also be useful in providing information when self-report techniques are often less useful (e.g., children), as well as with clients more open to projective as compared to self-report and interview methods. It is recommended that researchers study the incremental validity of projective techniques as compared to alternate methods, as well as consider the clinical efficacy and efficiency of projective techniques that incorporate suicide assessment information within the broader context of personality assessment.
Particularly lacking in the projective assessment literature on suicide is the utility of such methods with specific clinical populations and diverse populations. Few studies have investigated whether projective techniques are more or less useful with specific diagnostic groups (e.g., mood disorder vs. schizophrenia). No studies have specifically investigated the use of projective techniques in light of client diversity along dimensions of client social and economic status, ethnicity, religiosity, or sexual orientation. Researchers have also largely left gender unexamined as a factor potentially affecting the evaluation of suicidal ideation and self-harm. Lastly, physical disability, terminal illness, and head injury have been identified as mitigating factors in suicidal ideation (Orbach, 1997; Sa´nchez, 2001); however, no research could be found that investigated how these factors may influence the use of projective techniques with suicidal patients. Thus, the effect of client variables on projective methods in assessing suicidal ideation and behavior remains poorly understood, and further research on these factors is recommended.
CONCLUDING STATEMENTS
Projective techniques will naturally be most beneficial to clients when incorporated with other suicide assessment strategies, and clinicians are cautioned against relying on any single assessment method in evaluating a patient’s risk for suicide and self-harm. Several models for suicide assessment have suggested that the complexity of suicidal behavior can
be best understood as a combination of mental illness, altered phenomenological states, self-destructive processes, personality traits, current stressors, historical/background factors, social and environmental facilitators, suicide-specific behavior, and protective factors (Clark & Fawcett, 1992; Orbach, 1997; Sa´nchez, 2001). Given the complex nature of suicidal ideation and risk for self-harm, leading suicidologists have recommended that clinicians use multifactor and multimethod approaches to suicide risk assessment (Berchick & Wright, 1992; Berman & Jobes, 1991; Bongar, 1991; Lovett & Maltsberger, 1992).
Projective techniques may be most useful in assisting clinicians’ understanding of their clients’ long-term risk for selfharm, as well as assisting clinicians and patients in informing their decisions regarding treatment planning, including hospitalization (Comstock, 1992). As has been stated in this chapter, projective techniques remain in their infancy regarding suicide assessment, and it is recommended that further research explore the reliability, validity, and diagnostic efficiency of these instruments. With additional research, both the quality and variety of projective techniques used in screening and formal assessment of suicidal ideation and risk for selfharm may be enhanced. It is recommended that clinicians consider the convergent and divergent information provided through projective, self-report, and interview techniques and select assessment methods that will provide their client the greatest benefit depending on the assessment occasion. Lastly, it is recommended that mental health professionals maintain an awareness of the clinical, ethical, and legal issues surrounding the care of suicidal patients (see Bongar, 1991, 1992, 2001). To assist clinicians working with suicidal patients, additional resources on the assessment and treatment of suicidal individuals, as well as risk management and legal issues, have been included in the Appendix.
APPENDIX: RECOMMENDED READINGS AND RESOURCES
Assessment and Intervention
- Berman, A.L., & Jobes, D.A. (1991). Adolescent suicide: Assessment and intervention. Washington, DC: American Psychological Association.
- Bongar, B. (Ed.). (1992). Suicide: Guidelines for assessment, management, and treatment. New York: Oxford University Press.
- Freeman, A., & Reinecke, M.A. (1993). Cognitive therapy of suicidal behavior: A manual for treatment. New York: Springer.
- Leenars, A.A., Maltsberger, J.T., & Neimeyer, R.A. (1994). Treatment of suicidal people. New York: Taylor & Francis.
- Maris, R.W., Berman, A.L., Maltsberger, J.T., & Yufit, R.I. (Eds.). (1992). Assessment and prediction of suicide. New York: Guilford Press.
- Schneidman, E., Farberow, N.L., & Litman, R. (1994). The psychology of suicide: A clinician’s guide to evaluation and treatment. Northvale, NJ: Jason Aronson.
Risk Management/Legal Issues
- Baerger, D.R. (2001). Risk management with the suicidal patient: Lessons from case law. Professional Psychology: Research and Practice, 32, 359–366.
- Bongar, B. (2001). The suicidal patient: Clinical and legal standards of care (2nd ed.). Washington, DC: American Psychological Association.
Internet Resources
- American Association of Suicidology, www.suicidology.org.
- American Foundation for Suicide Prevention, www.afsp.org.
- NIMH Suicide Research Consortium, www.nimh.nih.gov/research.
REFERENCES
- Acklin, M.W., McDowell, C.J., Verschell, M.S., & Chan, D. (2000). Interobserver agreement, intraobserver reliability, and the Rorschach Comprehensive System. Journal of Personality Assessment, 74, 15–47.
- Adkins, K.K., & Parker, W. (1996). Perfectionism and suicidal preoccupation. Journal of Personality, 64, 529–543.
- Anastasi, A. (1988). Psychological testing (6th ed.). New York: Macmillan.
- Anders, A.L. (1998). The utility of the Hand Test in the assessment of suicide risk. Dissertation Abstracts International, 59, 1908B.
- Appellbaum, S.A., & Colson, D.B. (1968). A reexamination of the color-shading Rorschach test response and suicide attempts. Journal of Projective Techniques and Personality Assessment, 32, 160–164.
- Appellbaum, S.A., & Holzman, P.S. (1962). The color-shading response and suicide. Journal of Projective Techniques, 26, 155– 161.
- Arffa, S. (1982). Predicting adolescent suicidal behavior and the order of Rorschach measurement. Journal of Personality Assessment, 46, 563–568.
- Berchick, R.J., & Wright, F.D. (1992). Guidelines for handling the suicidal patient: A cognitive perspective. In B.M. Bongar (Ed.), Suicide: Guidelines for assessment, management, and treatment (pp. 179–186). New York: Oxford University Press.
- Berman, A.L., & Jobes, D.A. (1991). Adolescent suicide: Assessment and intervention. Washington, DC: American Psychological Association.
- Blatt, S.J., & Ritzler, B.A. (1974). Suicide and the representation of transparency and cross-sections on the Rorschach. Journal of Consulting and Clinical Psychology, 42, 280–287.
- Bongar, B. (1991). The suicidal patient: Clinical and legal standards of care. Washington, DC: American Psychological Association.
- Bongar, B. (1992). Suicide: Guidelines for assessment, management, and treatment. New York: Oxford University Press.
- Bricklin, B., Piotrowski, Z.A., & Wagner, E.E. (1962). The Hand Test. Springfield, IL: Charles C. Thomas.
- Broida, D.C. (1954). An investigation of certain diagnostic indications of suicidal tendencies and depression in mental hospital patients. Psychiatric Quarterly, 28, 453–464.
- Browning, D.L. (1986). Psychiatric ward behavior and length of stay in adolescent and young adult inpatients: A developmental approach to prediction. Journal of Consulting and Clinical Psychology, 54, 227–230.
- Clark, D.C., & Fawcett, J. (1992). Review of empirical risk factors for evaluation of the suicidal patient. In B. Bongar (Ed.), Suicide: Guidelines for assessment, management, and treatment (pp. 16– 48). New York: Oxford University Press.
- Clemence, A.J., Hilsenroth, M.J., Sivec, H.J., Rasch, M., & Waehler, C.A. (1998). Use of the Hand Test in the classification of psychiatric inpatient adolescents. Journal of Personality Assessment, 71, 228–241.
- Comstock, B.S. (1992). Decision to hospitalize and alternatives to hospitalization. In B. Bongar (Ed.), Suicide: Guidelines for assessment, management, and treatment (pp. 204–217). New York: Oxford University Press.
- Cooper, G.W., Bernstein, L., & Hart, C. (1965). Predicting suicidal ideation from the Rorschach: An attempt to cross-validate. Journal of Projective Techniques and Personality Assessment, 29, 168–170.
- Cramer, P. (1999). Future directions for the Thematic Apperception Test. Journal of Personality Assessment, 72, 74–92.
- Crosby, A.E., Cheltenham, M.P., & Sacks, J.J. (1999). Incidence of suicidal ideation and behavior in the United States, 1994. Suicide and Life-Threatening Behavior, 29, 131–140.
- Cutter, F., Jorgensen, M., & Farberow, N.L. (1968). Replicability of Rorschach signs with known degrees of suicidal intent. Journal of Projective Techniques and Personality Assessment, 32, 428– 434.
- Daston, P.G., & Sakheim, G.A. (1960). Prediction of successful suicide from the Rorschach test using a single sign approach. Journal of Projective Techniques, 24, 355–361.
- Drake, A.K., & Rusnak, A.W. (1966). An indicator of suicidal ideation on the Rorschach: A replication. Journal of Projective Techniques and Personality Assessment, 30, 543–544.
- Efron, H.Y. (1960). An attempt to employ a sentence completion test for the detection of psychiatric patients with suicidal ideas. Journal of Consulting Psychology, 24, 156–160.
- Exner, J.E. (1986). The Rorachach: A comprehensive system: Volume 1. Basic foundations (2nd ed.). New York: Wiley.
- Exner, J.E. (1993). The Rorschach: A comprehensive system (3rd ed., Vol. 1). New York: Wiley.
- Exner, J.E., & Wylie, J. (1977). Some Rorschach data concerning suicide. Journal of Personality Assessment, 41, 339–348.
- Eyman, J.R., & Eyman, S.K. (1992). Personality assessment in suicide prediction. In R.W. Maris, A.L. Berman, J.T. Maltsberger, & R.I. Yufit (Eds.), Assessment and prediction of suicide (pp. 183–201). New York: Guilford Press.
- Farberow, N.L. (1974). Use of the Rorschach in predicting and understanding suicide. Journal of Personality Assessment, 38, 411–419.
- Fisher, S. (1951). The value of the Rorschach for detecting suicidal trends. Journal of Projective Techniques, 15, 250–254.
- Fisher, S., & Hinds, E. (1951). The organization of hostility controls in various personality structures. Genetic Psychology Monographs, 44, 3–68.
- Fowler, J.C., Hilsenroth, M.J., & Piers, C. (2001). An empirical study of seriously disturbed suicidal patients. Journal of the American Psychoanalytic Association, 49, 161–186.
- Fowler, J.C., Piers, C., Hilsenroth, M.J., Holdwick Jr., D.J., & Padawer, J.R. (2001). The Rorschach suicide constellation: Assessing various degrees of lethality. Journal of Personality Assessment, 76, 333–351.
- Frank, G. (1994). On the prediction of suicide from the Rorschach. Psychological Reports, 74, 787–794.
- Frank, L.K. (1939). Projective methods for the study of personality. Journal of Psychology, 8, 389–413.
- Goldstein, D. (2000). Assessment of suicidal behaviors and risk among children and adolescents. Technical report submitted to NIMH under contract No. 263-MD-909995.
- Groth-Marnat, G. (1990). Handbook of psychological assessment (2nd ed.). New York: Wiley.
- Gutin, N.J. (1997). Differential object representations in inpatients with narcissistic and borderline personality disorders and normal controls. Dissertation Abstracts International, 58, 1532B.
- Hansell, A.G., Lerner, H.D., Milden, R.S., & Ludolph, P.S. (1988). Single-sign Rorschach suicide indicators: A validity study using a depressed inpatient population. Journal of Personality Assessment, 52, 658–669.
- Hertz, M.R. (1948). Suicidal configurations in Rorschach records. Rorschach Research Exchange, 12, 1–56.
524 Projective Assessment of Suicidal Ideation
- Hertz, M.R. (1949). Further study of “suicidal” configurations in Rorschach records. Rorschach Research Exchange, 13, 44–73.
- Hewitt, P.L., Flett, G.L., & Turnbull, D.W. (1992). Perfectionism and suicide potential. British Journal of Clinical Psychology, 31, 181–190.
- Hilsenroth, M., Fowler, C., Sivec, H., & Waehler, C. (1994). Concurrent and discriminant validity between the Hand Test pathology score and the MMPI-2. Assessment, 1, 111–113.
- Jobes, D.A. (1995). The challenge and promise of clinical suicidology. Suicide and Life-Threatening Behavior, 25, 437–449.
- Johnson, W.B., Lall, R., Bongar, B., & Nordland, M.D. (1999). The role of objective personality inventories in suicide risk assessment: An evaluation and proposal. Suicide and Life-Threatening Behavior, 29, 165–185.
- Kahill, S. (1984). Human Figure Drawings in adults: An update of the empirical evidence, 1967–1982. Canadian Psychology, 25, 269–292.
- Kendra, J.M. (1979). Predicting suicide using the Rorschach Inkblot test. Journal of Personality Assessment, 43, 452–456.
- Kenny, T.J., Rohn, R., Sarles, R.M., Reynolds, B.J., & Heald, F.P. (1979). Visual-motor problems of adolescents who attempt suicide. Perceptual and Motor Skills, 48, 599–602.
- Kestenbaum, J.M., & Lynch, D. (1978). Rorschach suicide predictors: A cross validation study. Journal of Clinical Psychology, 34, 754–758.
- Lehnert, K.L., Overholser, J.C., & Adams, D.M. (1996). The Cognition Rating Form: A new approach to assessing self-generated cognitions in adolescent sentence completions. Psychological Assessment, 8, 172–181.
- Leonard, C.V. (1973). Bender-Gestalt as an indicator of suicidal potential. Psychological Reports, 32, 665–666.
- Lester, D. (1970a). Attempts to predict suicidal risk using psychological tests. Psychological Bulletin, 74, 1–17.
- Lester, D. (1970b). Factors affecting choice of method of suicide. Journal of Clinical Psychology, 26, 437.
- Levinson, M., & Neuringer, C. (1972). Phenomenal environmental oppressiveness in suicidal adolescents. Journal of Genetic Psychology, 120, 253–256.
- Lilienfeld, S.O., Wood, J.M., & Garb, H.N. (2001, May). What’s wrong with this picture? Scientific American, 81–87.
- Lindner, R.M. (1946). Content analysis in Rorschach work. Rorschach Research Exchange, 10, 121–129.
- Litinsky, A.M. (1997). Dichotomous thinking as a sign of suicide risk on the TAT. Dissertation Abstracts International, 57, 4715B.
- Litman, R.E. (1967). Sigmund Freud on suicide. In E.S. Schneidman (Ed.), Essays in self-destruction (pp. 324–344). New York: Jason Aronson.
- Lovett, C.G., & Maltsberger, J.T. (1992). Psychodynamic approaches to the assessment and management of suicide. In B. Bongar (Ed.), Suicide: Guidelines for assessment, management,
and treatment (pp. 160–186). New York: Oxford University Press.
- Machover, K. (1949). Personality projection in the drawings of the human figure. Springfield, IL: Charles C. Thomas.
- Maltsberger, J.T. (1988). Suicide danger: Clinical estimation and decision making. Suicide and Life-Threatening Behavior, 18, 47–54.
- Maltsberger, J.T., & Buie, D. (1989). The psychological vulnerability to suicide. In D. Jacobs & H. Brown (Eds.), Suicide: Understanding and responding (pp. 59–71). Madison, CT: International Universities Press.
- Mann, J.J., Waternaux, C., Haas, G.L., & Malone, K.M. (1999). Toward a clinical model of suicidal behavior in psychiatric patients. American Journal of Psychiatry, 156, 181–189.
- McEvoy, T.L. (1974). Suicidal risk via the Thematic Apperception Test. In C. Neuringer (Ed.), Psychological assessment of suicidal risk (pp. 74–94). Springfield, IL: Charles C. Thomas.
- McNeish, T.J., & Naglieri, J.A. (1993). Identification of individuals with serious emotional disturbance using the Draw-A-Person: Screening procedure for emotional disturbance. Journal of Special Education, 27, 115–121.
- Meyer, G.J. (1997). On the integration of personality assessment methods: The Rorschach and MMPI-2. Journal of Personality Assessment, 68, 297–330.
- Meyer, G.J. (1999). The convergent validity of MMPI and Rorschach scales: An extension using profile scores to define response-character styles on both methods and a re-examination of simple Rorschach response frequency. Journal of Personality Assessment, 72, 1–35.
- Meyer, G.J., Riethmiller, R.J., Brooks, R.D., Benoit, W.A., & Handler, L. (2000). A replication of Rorschach and MMPI-2 convergent validity. Journal of Personality Assessment, 74, 175– 215.
- Murray, H.A. (1938). Explorations in personality. New York: Oxford University Press.
- Naglieri, J.A., & Pfeiffer, S.I. (1992). Performance of disruptive behavior disordered and normal samples on the Draw-A-Person: Screening procedure for emotional disturbance. Psychological Assessment, 4, 156–159.
- National Institute of Mental Health (2001). In harm’s way: Suicide in America. NIH Publication No. 01-4594. Retrieved from http:// www.nimh.nih.gov/publicat/harmaway.htm.
- Neuringer, C. (1965). The Rorschach test as a research device for the identification, prediction and understanding of suicidal ideation and behavior. Journal of Projective Techniques and Personality Assessment, 29, 71–82.
- Neuringer, C. (1974). Suicide and the Rorschach: A rueful postscript. Journal of Personality Assessment, 38, 535–539.
- Neuringer, C., McEvoy, T.L., & Schlesinger, R.J. (1965). The identification of suicidal behavior in females by the use of the Rorschach. Journal of General Psychology, 72, 127–133.
- Ngai, A. (2001). Representational world of the suicidal youth as depicted in the TAT. Dissertation Abstracts International, 61, 3854B.
- Orbach, I. (1988). Children who don’t want to live. San Francisco: Jossey-Bass.
- Orbach, I. (1997). A taxonomy of factors related to suicidal behavior. Clinical Psychology: Science and Practice, 43, 208–224.
- Pfeffer, C.R., & Richman, J. (1991). Human Figure Drawings: An auxiliary diagnostic assessment of childhood suicidal potential. Comprehensive Mental Health Care, 1, 77–90.
- Range, L.M., & Knott, E.C. (1997). Twenty suicide assessment instruments: Evaluation and recommendations. Death Studies, 21, 25–58.
- Rierdan, J., Lang, E., & Eddy, S. (1978). Suicide and transparency responses on the Rorschach: A replication. Journal of Consulting and Clinical Psychology, 46, 1162–1163.
- Roback, H.B. (1968). Human Figure Drawings: Their utility in the clinical psychologist’s armamentarium for personality assessment. Psychological Bulletin, 70, 1–19.
- Rohde, A.R. (1957). The Sentence Completion Method: Its diagnostic and clinical application to mental disorders. New York: Ronald Press.
- Rothberg, J.M., & Geer-Williams, C. (1992). A comparison and review of suicide prediction scales. In R.W. Maris, A.L. Berman, J.T. Maltsberger, & R.I. Yufit (Eds.), Assessment and prediction of suicide (pp. 202–217). New York: Guilford Press.
- Rotter, J.B., Lah, M.I., & Rafferty, J.E. (1992). Rotter Incomplete Sentences Blank: Manual (2nd ed.). San Antonio, TX: Psychological Corporation.
- Rotter, J.B., & Rafferty, J.E. (1950). Manual for the Rotter Incomplete Sentences Blank: College Form. New York: Psychological Corporation.
- Rydin, E., Asberg, M., Edman, G., & Schalling, D. (1990). Violent and nonviolent suicide attempts—a controlled Rorschach study. Acta Psychiatrica Scandinavica, 82, 30–39.
- Rydin, E., Schalling, D., & Asberg, M. (1982). Rorschach ratings in depressed and suicidal patients with low levels of 5-hydoxyindoleacetic acid in cerebrospinal fluid. Psychiatry Research, 7, 229–243.
- Sakheim, G.A. (1955). Suicidal responses on the Rorschach test: A validation study. Journal of Nervous and Mental Disease, 122, 332–334.
- Sa´nchez, H.G. (2001). Risk factor model for suicide assessment and intervention. Professional Psychology: Research and Practice, 32, 351–358.
- Sapolsky, A. (1963). An indicator of suicidal ideation on the Rorschach test. Journal of Projective Techniques and Personality Assessment, 27, 332–335.
- Schneidman, E.S. (1993). Suicide as psychache. Journal of Nervous and Mental Disease, 181, 145–147.
- Schneidman, E.S. (1996). The suicidal mind. New York: Oxford University Press.
- Schneidman, E.S., & Farberow, N.L. (1958). TAT heroes of suicidal and nonsuicidal subjects. Journal of Projective Techniques, 22, 211–228.
- Silberg, J.L., & Armstrong, J.G. (1992). The Rorschach test for predicting suicide among depressed adolescent inpatients. Journal of Personality Assessment, 59, 290–303.
- Sivec, H., & Hilsenroth, M. (1994). The use of the Hand Test with children and adolescents: A review. School Psychology Review, 23, 526–545.
- Smith, K. (1981). Using a battery of tests to predict suicide in a long-term hospital: A quantitative analysis. Journal of Clinical Psychology, 37, 555–563.
- Smith, K. (1983). Using a battery of tests to predict suicide in a long-term hospital: A clinical analysis. Omega: Journal of Death and Dying, 13, 261–275.
- Smith, K., & Eyman, J.R. (1988). Ego structure and object differentiation in suicidal patients. In H. Lerner & P. Lerner (Eds.), Primitive mental states and the Rorschach (pp. 175–202). Madison, CT: International Universities Press.
- Sternberg, D., & Levine, A. (1965). An indicator of suicidal ideation on the Bender Visual-Motor Gestalt Test. Journal of Projective Techniques and Personality Assessment, 29, 377–379.
- Taylor, D.A. (1984). Views of death from sufferers of early loss. Omega: Journal of Death and Dying, 14, 77–82.
- Tharinger, D.J., & Stark, K. (1990). A qualitative versus quantitative approach to evaluating the Draw-A-Person and Kinetic Family Drawing: A study of mood and anxiety disordered children. Psychological Assessment, 4, 365–375.
- Viglione, D.J. (1999). A review of recent research addressing the utility of the Rorschach. Psychological Assessment, 11, 251– 265.
- Virshup, E. (1976). On graphic suicide plans. Art Psychotherapy, 3, 17–22.
- Vivona, J.M. (1997). Suicidal ideation, object relations, and early experiences: An investigation using structural equation modeling. Dissertation Abstracts International, 57, 4731B.
- Wagner, E. (1983). The Hand Test manual (Rev. ed.). Los Angeles: Western Psychological Services.
- Weiner, I.B. (1961). Cross-validation of a Rorschach checklist associated with suicidal tendencies. Journal of Consulting and Clinical Psychology, 25, 312–315.
- Westen, D. (1991). Social cognition and object relations. Psychological Bulletin, 109, 429–455.
- Wood, J.M., Nezworski, M.T., & Stejskal, W.J. (1996). The Comprehensive System for the Rorschach: A critical examination. Psychological Science, 7, 3–17.
- Zalsman, G., Netanel, R., Fischel, T., Freudenstein, O., Landau, E., Orbach, I., et al. (2000). Human Figure Drawings in the evaluation of severe adolescent suicidal behavior. Journal of the American Academy of Child and Adolescent Psychiatry, 39, 1024–1031.
Projective Assessment of Disordered Thinking
JAMES H. KLEIGER
UNDERSTANDING DISORDERED THINKING 526 CONCEPTUALIZING DISORDERED THINKING 527 Theoretical Approaches 527 Categorical Approaches 530 Generic Thought Disorder Typology 531 PROJECTIVE METHODS FOR ASSESSING DEVIANT THINKING 531 Rorschach Inkblot Method 531
Lindzey (1961) indicated that projective techniques are both sensitive to covert or unconscious aspects of behavior and evocative of fantasy life. In particular, projective tests allow for the graphic symbolic representation of internal schemas of self and others, motivational issues, and significant areas of intrapsychic conflict. However, viewing projective testing only in this way limits its scope primarily to the assessment of “contents of the mind,” or mental dynamics, as opposed to psychic structure. In other words, by stating that projective techniques evoke fantasy, Lindzey emphasized content and dynamics over form and structure. This general tendency to view projective testing as a means for assessing the “what and why” that underlies behavior all but ignores its role in the assessment of the “how” of behavior. Inferences from projective techniques should not be limited to mental content (i.e., wishes, fantasies, motivation, conflicts, and self- and object representations) but should also concern formal or structural aspects of personality. For example, in using projective storytelling, inkblot, or drawing techniques, psychologists pay attention not only to what themes are portrayed by the story, inkblot, or drawing but also to how these themes are told, perceived, or drawn. Thematic issues are, of course, of great interest, but what about the coherence and degree of organization of the responses, stories, drawings, and so forth? The words are important but so is the music.
Coherence and organization of responses place us within the realm of ego functioning, or specifically the domain of thought organization. Although projective techniques provide an excellent means of assessing disturbed ideas or fantasies,
Projective Storytelling Techniques (TAT and CAT) 532 Figure Drawing Tests 533 Sentence Completion Tests 535 CONCLUSIONS 536 REFERENCES 536
they can be equally useful in explicating formal disturbances in perception and thought organization. However, before discussing this issue further, it is necessary to define what is meant by the term thought disorder. Following a brief discussion of the scope and concept of disordered thinking, I turn to how projective techniques can aid in identifying the nature and severity of clinical thought disturbances.
UNDERSTANDING DISORDERED THINKING
Fish (1962) defined thought disorder as a disturbance of conceptual thinking in the absence of serious brain diseases and in the presence of adequate intelligence. Harrow and Quinlin (1985) provided another simple definition stating that thought disorder describes a variety of diverse types of verbalization and thinking that are labeled by others as bizarre and idiosyncratic. A more comprehensive definition of the concept of thought disorder would be one that encompasses a broader perspective that includes not only traditional concepts such as impaired pace and flow of associations but also such factors as errors of syntax, word usage, syllogistic reasoning, inappropriate levels of abstracting, failure to maintain conceptual boundaries, and breakdown in the discrimination of internal perceptions from external ones. Such a definition comes closer to capturing the multidimensional nature of disturbances and thought organization. Described in a broad manner such as this, disordered thinking has been conceptualized and elaborated in a variety of ways, some of which have led to confusion and sparked disagreement and controversy over the decades.
Kleiger (1999) summarized a number of the controversial issues that have plagued the concept of thought disorder. Is thought disorder better understood as a “speech or language disorder”? Is it specific to and pathognomic of schizophrenia? Furthermore, is thought disorder a dichotomous entity or a continuous dimension? Finally, is it synonymous with the concept of psychosis? Most of these issues have been largely laid to rest, but some still generate confusion and disagreement among clinicians and researchers. For example, despite some persuasive arguments of those who prefer to view thought disorder as a “speech disturbance,” the term thought disorder is a staple in the lexicon of mental health professionals. More settled are the debates about the diagnostic specificity of thought disorder and whether it is a continuous or discrete variable. It is generally accepted that varying degrees and manifestations of disordered thinking occur in a range of clinical syndromes (Kleiger, 1999). No longer is disordered thinking considered to be specific to schizophrenia but it is seen to occur in bipolar, borderline, and post-traumatic syndromes, to name but a few. The relationship between the constructs thought disorder and psychosis is, perhaps, less clear and depends upon how each term is defined. Are they synonymous or is one concept subsumed under the other? If the latter is the case, which concept is subsumed under the other? The best way to address this confusing question is to review some of the ways in which thought disorder has been conceptualized.
CONCEPTUALIZING DISORDERED THINKING
There are a number of conceptual models for understanding thought disorder. Each offers something unique in conceptualizing the underlying psychological processes associated with disordered thought. Taken together, these models can contribute to a set of molar principles for understanding thought disorder independent of any specific testing instrument, scale, or scoring system. In other words, one way of exploring the use of projective tests in the assessment of disordered thinking is to develop a superordinate way of conceptualizing thought disorder that could be accommodated to different projective techniques. The goodness of fit in adapting this set of principles would then depend on the unique stimulus features and demands of each projective instrument.
What follows is a review of some conceptual models for understanding thought disorder. This review is by no means exhaustive. Although the concept of thought disorder is more frequently studied these days from a neuropsychological perspective, the models reviewed here focus on disordered thinking as experience-near psychological phenomena that occur in a range of clinical situations, the manifestations of which can be assessed by different psychodiagnostic techniques.
Theoretical Approaches
Several theory-based approaches have been developed to establish a conceptual basis for understanding of thought disorder. Although most of these models were established primarily for use with the Rorschach, their linkage to a theory independent of the Rorschach makes them potentially useful with other instruments as well.
Thought Disorders of Form Versus Content
The psychiatric study of thought disorder generally makes the distinction between thought disorders of “form” versus “content.” Distinguishing between structure or process, on the one hand, and content, on the other, is an important consideration in the study of behavior and psychological experience. In terms of thought disorder, perhaps the best way to make the distinction is to consider that people may either express “crazy” ideas in a clear and coherent manner, or they may express mundane, reality-oriented ideas in a peculiar, disorganized, or incoherent manner. The ideas may be absurd or highly deviant, or the way in which they are expressed may be disturbed. In many cases, disordered thinking is manifest both in the content as well as the expressive form or structure of the ideas.
Rapaport’s Concept of “Distance”
For Rapaport (Rapaport, Gill, & Schafer, 1944–1946), assessing thought disorder from Rorschach verbalizations was based on his concept of distance from the inkblot. Rapaport believed that thought processes were always tied to the perceptual reality of the inkblot. Adaptive, reality-based thinking depends on the smooth interdigitation of perceptual and associational processes. In other words, the associations set in motion by the inkblot must not stray too far, or be too distant from, the perceptual reality of the inkblot. If associative processes are too far removed, or distant, from the inkblot, the subject has disregarded the perceptual reality in front of him or her. On the other hand, rigid attunement to the perceptual features of the inkblot may lead a subject to regard it as too real, hence failing to maintain an appropriate distance or “as if” attitude toward the inkblots.
Although Rapaport made passing reference to the concept of distance in discussing two other projective techniques, the Word Association Test and the Thematic Apperception Test (TAT), he was careful to restrict the meaning of this concept to the Rorschach. According to Rapaport, the key to understanding pathological verbalizations and their underlying thought processes was to not lose sight of the reality of the Rorschach situation, or, in this case, the perceptual reality of the inkblots. Fabulized combinations, confabulations, odd verbalizations, contaminations, and autistic logic could all be conceptualized as manifestations of either a pathological loss or increase of distance from the inkblots. Thus, for Rapaport, the concepts of loss and increase of distance from the inkblots were a cornerstone for understanding thought organization and served as a yardstick for measuring disturbances in thinking.
Schuldberg and Boster (1985) criticized the lack of conceptual clarity in Rapaport’s model of pathological thinking on the Rorschach. Since the concept of distance was the theoretical stanchion that supported Rapaport’s understanding of disordered Rorschach responses, Schuldberg and Boster conducted an empirical analysis of the data on which this concept was based. According to their factor analysis, the thoughtdisordered responses of Rapaport’s subjects did not form a unidimensional measure of pathological thinking. Instead, they determined that two dimensions provided a reasonable economical representation of the structure of Rapaport’s thoughtdisorder scoring categories and his concept of distance.
The first dimension contained scoring categories having to do with objective versus personalized meaning. The low end of this dimension (Dimension 1) was typified by confusion responses, in which the subject struggled to find the real meaning inherent in the inkblots. Subjects who gave confusion responses had difficulty interpreting the inkblots and instead attempted unsuccessfully to recognize the “pictures” that they believed the inkblots reflected. The high end of Dimension 1 is represented by self-reference and incoherence responses, two categories that reflect the intrusion of unrelated personal associations into the task. Thus, Dimension 1 contrasts responses that reflect an overly literal approach to the blots (taking the inkblots as something “real” to be recognized) with responses that reflect the infusion of overly personalized (and idiosyncratic) meaning into the response process. Other examples of scores low on this dimension include position responses, reference ideas, and perseveration. Other scores at the high end of Dimension 1 are neologisms and autistic logic.
Dimension 2 is related to verbal productivity and refers to rigid versus fluid sets in approaching the task. Responses at the low end of this dimension reflect excessive rigidity in being able to break a mental set to create new ideas. Perseveration and relationship verbalizations both reflect rigidity, stimulus boundedness, and set-shifting difficulties. At the high or fluid end of Dimension 2 are scoring categories that reflect a departure from the stimulus field and a focus on emotionally charged or overly specific associations. Confabulations and absurd responses are examples of responses that have little grounding in the reality of the inkblot. Thus, categories low on this dimension reflect an excessive narrowing or rigidity in associational and attentional processes, whereas categories on the high end reflect a disorderly, unstable, and overly elaborated response process.
Schuldberg and Boster further determined that the global amount of thought disorder manifested on the Rorschach is more closely associated with Dimension 1 than with Dimension 2. This correlation implies that disordered thinking on the Rorschach reflects primarily those efforts to interpret the blots in either an inappropriately concrete manner or an overly personalized and idiosyncratic manner.
In terms of differential diagnosis, Schuldberg and Boster viewed schizophrenic concreteness on the Rorschach as an inability to shift sets away from one focus of attention (low Dimension 2) and also by a stimulus boundedness or tendency to ascribe literal meaning to the inkblots (low Dimension 1). Scores high on Dimension 2 reflect fluid sets, characterized by overly elaborated responses that are independent of the stimulus qualities of the inkblot. Schuldberg and Boster indicated that this flamboyant style has been shown to be diagnostic of borderline psychopathology and manic conditions.
Before leaving the subject of “distance,” it is important to take note of Rapaport’s other usage of the term distance when talking about the process of association and concept formation (Rapaport et al., 1944–1946). Although related to the Rorschach concept as discussed above, Rapaport described “close” and “distant” associative reactions to stimulus words on the Word Association Test. Essentially, close reactions occurred when the subject’s response to the stimulus word was too closely or literally tied to the stimulus word. Again, the concept of stimulus boundedness has some relevance here. In contrast to close reactions, Rapaport defined distant reactions as being unrelated to the stimulus word.
Thus, we have an additional nuance to Rapaport’s concept of distance that may be useful in thinking about the manifestations of disordered thinking on a wider range of projective testing instruments.
Holt’s Primary Process (PRIPRO)
Holt (1956, 1977; Holt & Havel, 1960) established a theoretically based Rorschach scoring system to assess primary process manifestations along with aspects of ego control and defense. With close to 100 individual scoring variables grouped together across three broad dimensions, Holt designated his scoring system as a research tool as opposed to a clinical instrument. Each of the three dimensions corresponds to a different aspect of primary process thinking. First, since primary process thinking is characterized by its wishful quality, Holt constructed a group of “content variables” to reflect the degree of primary process wishfulness (i.e., libidinal or aggressive) present in the content of each response. Secondly, primary process thinking is defined by unique structural characteristics, which led Holt to modify and extend Rapaport’s list of Rorschach scoring categories for formal thought disorder and develop his own set of “formal” or structural variables. Finally, the emergence of primary process content or formal manifestations of primary process thinking prompts either effective or ineffective defensive and control efforts, which are measured by Holt’s third category, “control and defense variables.” Holt’s system is unique in its development of categories for assessing primitive aspects of response content as well as defensive or adaptive aspects of the response.
Weiner’s Ego Disturbance Model of Thought Disorder
Weiner’s (1966) psychodiagnostic study of schizophrenia was based on the premise that the diagnosis of schizophrenia is essentially a diagnosis of impaired ego functioning. Weiner indicated that effective secondary process thinking requires the integration of a number of ego capacities, including cognitive focusing, reasoning, concept formation, and relation to reality. Impairment in any combination of these may gain expression in different forms of thought disorder. By linking thought disorder to disturbances in ego functioning, Weiner freed the concept of disordered thinking from any one specific psychological testing instrument. The categories Weiner chose are briefly presented here.
1. Cognitive focusing. Efficient thinking necessitates an ability to scan information selectively, to separate essential from nonessential information, and to exclude that which is irrelevant to one’s focus. Weiner divided cognitive focusing difficulties into those that he called “failure to establish a focus” and those he referred to as “failure to maintain a focus.” Failure to establish a focus includes difficulties selecting for attention the most relevant aspects of the stimulus field and adjusting one’s attention accordingly. A subject who fails to establish a cognitive focus may also produce perseverative responses. Here the subject is unable to shift attentional focus as the qualities of external stimuli change. Without this ability to alter focus, one may be doomed to echoing previous responses, even if these are no longer relevant to the demands of the present stimulus situation.
Failure to maintain a focus consists of the intrusion of irrelevant external or internal stimuli onto a previously established set, which may lead to the overt expression of idiosyncratic associations or erratic flow and pace of associations. Idiosyncratic associations may actually reflect a deficiency in screening as the individual is unable to prevent deviant associations from intruding into the response.
2. Reasoning. Reasoning is a critical aspect of thinking in which one attempts to draw inferences from one’s experiences and observations and look for logical connections between objects and events in the environment. Weiner organized reasoning disturbances under the three subcategories of “combinative thinking,” “circumstantial thinking,” and “overgeneralized thinking.”
Combinative reasoning is based on the primary process mechanism of condensation, in which ideas and perceptions are combined in a manner that is illogical and unrealistic. One who combines ideas and images unrealistically may conclude that two things that simply occur together in time and space belong together in some conceptually meaningful way. In combinative reasoning, the perceptual relationship between discrete elements overshadows any consideration of the conceptual reality or appropriateness of the relationship.
Circumstantial reasoning involves basing conclusions on incidental or nonessential details. Related to the older concepts of “predicate thinking” (von Domarus, 1944) or “paleological thinking” (Arieti, 1974), circumstantial thinking runs contrary to the rules of formal syllogistic reasoning. The formation of stereotypes (e.g., “Basketball players are tall; he is tall; therefore he is a basketball player” [Kleiger, 1999, p. 229]) is an example of a normative, nonpsychotic type of circumstantial reasoning.
Over-generalized reasoning involves overinterpreting the meaning of data and forming conclusions based on minimal evidence. Part of this process may involve elaborating or embellishing one’s observations beyond what the properties of the stimulus can justify. In over-generalized reasoning, one bases conclusions on minimal evidence, often reading an inappropriate degree of meaning into a more or less neutral or ambiguous stimulus situation.
3. Concept formation. Concept formation involves the ability to interpret experience at appropriate levels of abstraction. Related to some extent to Rapaport’s concept of distance, impairments in conceptual thinking reveal themselves in either the extremes of concreteness or overinclusiveness. In either case, the individual has difficulty focusing on the most salient and relevant features of a given situation. Conceptual categories are made up of items that are related to one another. Conceptual spans can be overly narrow, being made up of too few members, or overly loose or inclusive, being composed of too many unrelated members.
4. Reality testing. More related to perception than to thinking, per se, reality testing involves the capacity to perceive and interpret reality accurately. Is the individual able to judge the origin of a stimulus or whether it emanates from an intrapsychic or environmental source? One measure of reality testing is to compare an individual’s perception of a stimulus to what is conventionally perceived by most people. Individuals who have trouble perceiving what most people can are said to have problems with reality testing.
Categorical Approaches
At a lesser level of abstraction than the theoretical approaches of Rapaport, Holt, and Weiner are categorical approaches to describing different types of disordered thinking. Two classification systems are presented. The question for present purposes is whether these may assist in the assessment of thought disorder with projective tests.
Psychiatric Typology
Andreasen’s Scale for the Assessment of Thought, Language, and Communication (TLC) (Andreasen, 1978) consists of definitions for rating the severity of 18 subtypes of formal thought disorder. Andreasen preferred to subdivide the realm of thought disorder into three categories, which she called “communication,” “language,” and “thought disorders.” She believed that many subtypes of communication disorders resulted when the speaker failed to follow conventional rules that are used to make it easier for listeners to understand what is being said. Among the communication disorders, Andreasen listed (1) Poverty of Speech Content, (2) Pressured Speech, (3) Distractible Speech, (4) Tangentiality, (5) Derailment or Looseness, (6) Stilted Speech, (7) Echolalia, (8) Self-Reference, (9) Circumstantiality, (10) Loss of Goal Directedness, (11) Perseveration, and (12) Blocking.
Andreasen reserved the term language disorders for those pathological instances in which the speaker violated syntactical and semantic conventions that guide language usage. Included among the language disorders were (1) Semantic Approximation, (2) Neologisms, (3) Incoherence, and (4) Clanging. Finally, Andreasen used the term thought disorder for those situations in which thinking by itself appeared to be deviant. Examples of thought disorder, per se, included (1) Poverty of Speech, in which thought does not seem to occur, and (2) Illogical Processes of Inference Making.
Rorschach Thought Disorder Factors
Johnston and Holzman (1979) initially developed the Thought Disorder Index (TDI) to assess disordered thinking in schizophrenia. Holzman and his colleagues later revised and expanded the scoring system to assess thought disturbances in a variety of clinical syndromes (Shenton, Solovay, & Holzman, 1987; Solovay, Shenton, & Holzman, 1987). Comprised of 23 discrete scores, weighted according to four levels of severity, the TDI is a complex Rorschach system that has been used successfully in numerous empirical investigations of thought disorder and psychopathology. The TDI was also originally used with both the Rorschach and verbal subtests of the WAIS, thus serving as a precedent for applying this Rorschach-based method for identifying disordered thinking to other psychological tests.
In order to study qualitative features of various forms of thought disorder, Holzman and colleagues looked at four sets of TDI factors that were derived by different statistical methods (Shenton et al., 1987; Solovay et al., 1987). One method, a principal components analysis with a variance maximization rotation, yielded a set of six conceptually meaningful molar categories described as follows.
1. Combinative thinking reflects an inappropriate integrative activity, in which separate details of the inkblot are synthesized without sufficient regard to the reality of the relationship. This is Weiner’s “combinative reasoning” category.
2. Idiosyncratic verbalization includes scores reflecting odd word usage.
3. Autistic thinking includes scores having to do with autistic logic (predicate thinking or Weiner’s “circumstantial reasoning”) and incoherence.
4. Fluid thinking refers to scores, such as Contamination and Fluidity, which reflect a problem maintaining stable perceptual and conceptual boundaries.
5. Absurdity is made up of scores such as Neologisms and Absurd Responses.
6. Confusion includes scores that reflect the subject’s confusion or inadequate efforts to formulate a coherent response.
In contrast to the complexity of the TDI, the Comprehensive System (Exner, 1993) offers a more economical approach to classifying thought disorder with seven specific scoring types and four molar categories. Exner, Weiner, and Schuyler (1976) described four categories of unusual verbalizations that included Deviant Verbalizations, Inappropriate Combinations, Inappropriate Logic, and Perseveration.
1. Deviant verbalizations include two types of scores in which distorted language usage, inappropriate verbal intrusions, or rambling circumstantial verbalization characterizes the response.
2. Inappropriate combinations include three types of scores in which blot details are combined or condensed in such a way as to produce unrealistic features on an object or implausible relationships between objects or between an object and its activity.
3. Inappropriate logic includes only one score that reflects the use of strained or unconventional reasoning to justify a response.
4. Perseveration reflects three subtypes of responses in which the subject gives two or more identical answers either to the same card or to different cards.
One potential difficulty in using the Rorschach is that different approaches use different scoring systems. Often the language of one system does not translate smoothly into the language of the other. Thus, using a generic, “nondenominational” typology, such as the one presented next, potentially offers clinicians a set of useful categories that are not linked specifically to any one scoring system. All of the categories of disturbed thinking represented in this typology capture the full range of deviant reasoning and verbalizations found in Rorschach responses.
Generic Thought Disorder Typology
The following typology borrows from established Rorschach categories but is also an attempt to be free of any instrument or specific scoring system and instead describe a generic thought disorder typology that can fit with the language and level of abstraction of testing and can be applied to a wider range of clinical instruments. Thus, in an effort to capture some of the Rorschach-derived categories but de-link them from the Rorschach, per se, the following typology of forms of disordered thinking is presented.
1. Idiosyncratic language ranges from mild to severely deviant verbalizations that include odd and stilted word usage and expressions, malapropisms, and neologisms.
2. Combinative thinking includes the combinatory and inappropriate combination categories described previously. Here the subject pays more attention to the perceptual relationship (proximity in space or time) than to the conceptual appropriateness of this perceived relationship.
3. Overly inferential thinking reflects the inappropriate attribution of specific detail or meaning that goes beyond and cannot be justified by the reality of the testing stimulus. The subject wanders far afield, or becomes “increasingly distant,” from the reality anchors of the testing stimulus. Rapaport’s term “confabulation” (Rapaport et al., 1944–1946) best captures this process but, unfortunately, has been used in too many different contexts to provide precise meaning anymore.
4. Vague and confused thinking reflects the subject’s own confusion in attempting to interpret and produce a response to a testing stimulus. Confused responses range from milder forms of vagueness, in which there is a poverty of expressed meaning in the response, to more severe examples of confused thinking, in which the subject becomes manifestly confused and perplexed as he or she attempts to respond to the testing stimulus or test instructions.
5. Condensed and fluid thinking captures a more severe collapse of boundaries between inherently separate frames of reference so that conceptual and/or perceptual boundaries are no longer maintained. The properties of the separate ideas or images begin to penetrate or are superimposed upon one another so that the proper distinction between them is lost.
6. Paleological reasoning is Arieti’s (1974) term for predicate or circumstantial thinking in which the subject explicitly demonstrates a loss of syllogistic capacity. Here the subject reaches an illogical conclusion with immediacy and conviction, while ignoring more relevant or discrepant details.
7. Impoverished and concrete thinking reflects a loss of abstract attitude (Goldstein & Scheerer, 1941) and representational capacity wherein the subject becomes bound to the concrete nature of the testing stimulus. Rapaport’s concept of a “loss of distance” captures this type of thinking.
8. Perceptual inaccuracies include overt and sometimes subtle misperception of details in the testing situation such that the subject bases his or her response more on idiosyncratic personal factors than on consensually valid perception of the testing stimuli.
PROJECTIVE METHODS FOR ASSESSING DEVIANT THINKING
The remainder of the chapter will focus on specific projective techniques and the assessment of thought disorder, with emphasis on applicability of the previously described generic typology.
Rorschach Inkblot Method
As indicated previously, there are two contemporary Rorschach approaches for scoring thought disorder manifestations. The Special Scores of the Comprehensive Rorschach System (Exner, 1993) and the Thought Disorder Index or TDI (Johnston & Holzman, 1979) both assess a range of deviant thought and speech elements embedded in verbalizations and reasoning used to justify a Rorschach response. Both instruments were developed in the mid-1970s but had relatively separate developments over the last several decades. Exner’s Comprehensive System is the most commonly used approach for administering, scoring, and interpreting the Rorschach, while the TDI was developed as a research instrument and, as such, has made fewer inroads into clinical assessment practice.
The TDI is made up of 23 different forms of thought disorder, scored at four levels of severity (.25; .50; .75; and 1.0). A more complex instrument to learn, the TDI is useful for identifying subtle differences among different groups of psychotic subjects, aiding in differential diagnosis of psychotic disorders. Interrater reliability is relatively good for ratings across different severity levels, with interclass correlations ranging from .72 to .77 (Coleman et al., 1993). Apart from its being a difficult instrument to learn, one drawback of the TDI is that it was developed using the Rapaport method of Rorschach administration, which differs from the standards used by the more popular Comprehensive System. Nonetheless, the TDI is viewed not only as a robust measure of thought disorder but as an instrument sensitive to identifying differential diagnostic patterns among different groups of psychotic subjects.
By contrast, the Special Scores of the Comprehensive System offer a much crisper and more economical approach to identifying major thought disorder categories. Four major categories comprising seven different scores (eight if CON-FAB is included) can be scored according to level of severity (Level 1, mild slippage; Level 2, moderate and severe). By reducing the number of categories, the Comprehensive System ensures better interscorer reliability and ease of learning. Different scores are weighted according to their level of severity and entered into the recently developed Perceptual-Thinking Index (PTI). The PTI is an improvement of the former Schizophrenia Index (SCZI), which proved to be inadequate as a specific diagnostic indicator. The SCZI yielded many false positives, as nonschizophrenic subjects with other forms of psychoses, trauma, or personality disorders often score positively on this index. Replacing the SCZI with the PTI recognized the importance of separating primary from secondary diagnostic inferences (Exner, 2000). The PTI is a measure of the severity of psychotic thought, as opposed to an index that is diagnostically specific to one particular clinical syndrome.
Projective Storytelling Techniques (TAT and CAT)
Projective storytelling techniques are usually added to the testing battery in order to assess relational paradigms and areas of conflict that are not consciously available to the subject. All too often, clinicians make literal or symbolic inferences about these issues based solely on the content of the stories. However, the importance of paying attention to structural aspects, regardless of content, was recognized by Rapaport (Rapaport et al., 1944–1946). Rapaport not only believed that the distinction between “projective” and “objective” tests was meaningless but that the projective hypothesis could be applied to any procedure. Furthermore, he held that all testing techniques could assess the organizing principles of behavior or the psychological structure of the person. With that in mind, he described several kinds of TAT verbalizations and response process variables indicative of schizophrenia. (Keep in mind that no one writing during Rapaport’s era spoke directly about “thought disorder,” per se, which was understood as a pathognomic and specific symptom of schizophrenia. The study of disordered thinking was incidental to a broader investigation of schizophrenia.)
Rapaport’s TAT variables can be divided into those having to do with response content (what the story is about) and those pertaining to the form or structure of the response (how the story is told). Some of Rapaport’s indicators of paranoia and schizophrenia are listed in the next two sections.
Content Variables
1. Unacceptable content. This is similar to Holt’s PRIPRO scales that assessed highly charged primary process content, including tabooed themes of raw aggression and sexuality.
2. Withdrawal content. Included here are themes reflecting a schizoid withdrawal from the world into an autistic state.
3. Delusional-like content. Direct reference to themes suggesting delusions of external control, paranoia, persecution, jealousy, erotomania, or grandiosity.
4. Bizarre fantasies in the content. Thematic content reflecting unrealistic events or capacities may signal a potential for delusional thinking and reality-testing difficulties.
Structural Variables
1. Deducing the motives of the examiner or artist. Subjects may openly wonder what the examiner is looking for or why he or she selected certain cards for them. Interest in why the examiner is making a verbatim record of the subject’s responses may also reflect a heightened interest in what is going on in the mind of the examiner.
2. Extended inferences. The subject who feels compelled to prove his inferences by focusing on subtle details in the pictures or who forms major conclusions based on insignificant nuances may be revealing deficits in focusing and reasoning.
3. Overelaborate symbolism. This can be considered both/ either a content or structural variable. Here the subject attributes overly abstract meaning to objects or actions in the picture in a manner that is both arbitrary and highly idiosyncratic. The subject is having difficulty interpreting the picture at an appropriate level of abstraction and maintaining an appropriate distance from the picture and task. He or she ascribes symbolic significance to aspects of the cards that seem idiosyncratic and arbitrary. Rapaport (Rapaport et al., 1944– 1946) indicated that Cards 8 and 10 were especially prone to evoking symbolic themes and gave the following example of such a response to Card 8:
The couple represents love, the figure on the right is the mother of the couple and the grandmother of the child, and she and the child represent continuous flow of renewal of life through the love forces . . . I think that it is implied that it is through the female side. I think it is possible that the husband, the man, wants to control life through the child and that the wife feels their love is enough and that the child will be trained by the institutions of civilization as represented by the clothed mother. I think the father would want to train it as an individual rather than as a member of society but the father will have completed his function in the propagation of the child. (Rapaport et al., 1944–1946, p. 450)
4. Peculiar turns in the content. Stories in which the plot shifts in nonsensical ways may reflect organizational difficulties and problems maintaining focus and screening out intruding material. In the TDI, the score “looseness” is given to responses that reflect such a loss of cognitive focus, in which the subject’s associations depart from the task at hand and become tangential or irrelevant. The following Card 5 response is an example of such looseness or loss of focus.
This lady has come down stairs to check who’s in her room.
When she opens the door, she sees no one but only sees the light left on by one of her children probably. So there is nothing to worry about, and she goes back to her room to sleep. The whole house probably blows up when she shuts off the lights because someone snuck in to rob her and planted a bomb. He worked for the IRA and was a terrorist and was sneaking around the neighborhood to find out people he didn’t like.
5. Vague generalities in the content. Again, one can view this as either a disturbance in the form or content of the response. Just as a Rorschach response can reflect vague and confused thinking, TAT stories may also demonstrate the subject’s confusion in finding any coherent meaning in the card. Instead, we find vague generalities and redundant formulations that add little, if anything, to the story. Subjects may also get mixed up in their stories and either indicate their confusion explicitly or make statements that are contradictory in nature. For example, note the redundancy, poverty of meaning, and confusion in temporal frame of reference at the end of the following Card 3BM story.
We’ll call her Mary. Yes, Mary is home from a long day at work. She works long hours and has just come home, probably home or it could be somewhere else she has come. She is home after working all week or for much of the day and has come into her room because she is so tired after working. She looks like she is tired because she is flopping down or is lying down or is just sitting after a long day. I’m not sure what she would be thinking, other than what a long day she has had or when she should come home from work, if she hasn’t already come home.
6. Disjointedness in organization. The organization of the story may become loose, fragmented, or incoherent to such an extent that the listener may have difficulty tracking the theme or plot.
7. Arbitrariness. Arbitrary elements are introduced into the story, which may take on an absurd quality in which the subject introduces issues or actions that are not justified by the picture.
8. Story continuations. Story continuations on the TAT are more common variants of the “relationship verbalizations” that occur on the Rorschach. Here, the subject links each story together, referring back to the original characters and action from an earlier card. Rapaport cautioned, however, that normal and neurotic subjects may link stories together by choice, whereas those with schizophrenia do so because they assume that the pictures need to go together.
9. Peculiar verbalizations. Finally, perhaps the most common manifestation of disordered thinking is the introduction of odd or stilted words or expressions into one’s story. As with the Rorschach, the TAT/CAT provides a narrative base reflecting idiosyncratic language and word usage that may signal potential thought disorder.
Figure Drawing Tests
Because of the nature of the task, there has been less attention paid to manifestations of disturbed thinking on projective drawing tasks. Unlike almost all other projective techniques, the data from projective drawing tests is nonverbal in nature. Narrative expression may have a small role in drawing tasks if the examiner specifically conducts some kind of inquiry after the subject has drawn the figures, but a rich verbal dataset is largely absent in most projective figure drawing techniques.
However, despite this obvious difference from verbally mediated tests, figure drawings may also be evaluated in terms of both structure and content. Structural variables concern the style or form in which the drawing was executed. Dimensions like size, placement on the page, line quality, degree of detailing, perspective, shading, erasure, and work overall pertain to how the drawing was executed. In contrast, content-based approaches to interpretations usually concern specific aspects of the body, house, or tree.
Handler (1985) reviewed both structural and content aspects of the Draw-A-Person that might indicate a more severe, psychotic level of disturbance. For example, extremely discontinuous line quality may reflect problems with reality content and bizarre thoughts. Lack of sufficient detail or bizarre details may be indicative of psychosis (McElhaney, 1969). Other structural features associated with possible psychosis include disorganized placement on the page, distortions and omissions, and transparencies. In terms of specific drawing content suggestive of disordered thinking or psychosis, Handler included the omission of facial features and the emphasis on ears and eyes. In particular, emphasis on eyes and ears has been associated with paranoid trends, ideas of reference, or even auditory hallucinations (Buck, 1966; DiLeo, 1973).
However, caution is always indicated when inferring psychological meaning from aspects of a person’s drawing. Especially for children, one must be aware of developmental factors when making interpretations of either the form or content of a drawing. For adults and children alike, ascribing the same meaning to each structural or content variable may lead to an uncritical sign approach that overshadows a conceptual appreciation of the psychological processes underlying the aspects of the drawing in question.
The question remains as to whether formal aspects of figure drawings can be organized into a framework that gets away from the one-dimensional sign approach that has typically been used (and misused) when interpreting projective figure drawings. The following categories may help provide a framework for thinking about aspects of figure drawings that might indicate disordered thinking.
1. Deviant verbalization. Clearly this category is only relevant if one is introducing a narrative inquiry into what is essentially a nonverbal task. Kissen (1981) has such a modification, in which he asks the subject a series of open-ended questions about his or her drawings.
2. Combinative drawings. Combinative thinking occurs when one assumes a meaningful relationship between two events or objects that occur together in time or space. In figure drawings, there is no standard, objectifiable stimulus situation to which the subject is reacting in the same way that he or she reacts to an inkblot, a picture, or an interpersonal transaction. Instead, the subject is asked to construct a representation of a person, house, or tree. The stimulus, if you will, is internal. Incongruous combinations reflecting hybrid creatures (e.g., humans with an inappropriate number of body parts, human and animal combinations, or animate-inanimate composite forms) may certainly be observed; but they are, by comparison, rarer and more flagrant indicators of disturbed thinking and reality testing. Unlike the passive “loss of distance” on the Rorschach, in which the subject mistakes a perceptual relationship for a conceptual one, inappropriate combinations in drawings may be the result of a more active process of distortion. Of course, evaluating the subject’s intent is always crucial. Is the incongruous combination in a human figure drawing a product of artistic motivation or the wish to defy or shock? Is the subject trying to be playful or responding to some inner imperative that is overly private and laden with idiosyncratic personal meaning?
3. Fluid and condensed drawings. The best example of contaminatory thinking on a human figure drawing test is transparencies. Widely viewed as a near pathognomic sign of psychotic thinking, transparencies occur when the subject fuses incompatible frames of reference, in this case internal and external. However, there seem to be various levels of transparencies reflecting differing degrees of reality distortion (Machover, 1949). Drawings in which the lines of the figure are apparent beneath the clothing may reflect immaturity, carelessness, lack of attention to detail, or poor judgment. However, drawing genitals under clothing requires a more active distortion of reality. Finally, when one draws internal organs inside the figure, one is collapsing an external view with an internal one, revealing, perhaps, the most serious sign of disordered thinking and reality testing.
4. Impoverished and simplified drawings. Assuming normal intelligence and appropriate level of development, overly simplified drawings often reflect a reduction of energy or interest in the task that may be associated with any number of things. Small and undifferentiated figures with little detail may reflect a loss of interest or motivation such as that observed in depressive disorders. However, the same features may represent negative signs of thought disorder, reflecting a general constriction and impoverishment in thinking.
5. Confused drawings. Subjects who express hesitancy and doubt about their drawings may struggle with what Piotrowski (1937) termed “impotency and perplexity,” in which the individual gives a response despite the recognition that it is inadequate or shows mistrust in his or her ability to carry out the instructions. Clearly, when talking about this kind of disturbed process, one needs to consider the presence of underlying brain impairment.
6. Perceptually inaccurate drawings. Unlike the hybrid figures that reflect an active combinative process, some drawings may simply be fragmented and poorly integrated. Like the confused and overly simplified drawings, poorly integrated drawings, with missing or misplaced details, are general indications of brain damage (Lezak, 1976). Included under this category would be broken contours, which Weiner (1966) interpreted as a failure to establish ego boundaries related to an impairment in the sense of reality. Broken contours are a more meaningful sign of cognitive impairment (whether of a psychological or organic nature) when the subject appears to have taken his or her time to complete the drawing.
Sentence Completion Tests
Although sentence completion tests (SCTs), unlike projective drawing tasks, are verbally mediated techniques, there is a dearth of literature that has looked at manifestations of thought disorder on these tests. This may be due to several factors: (1) SCTs are not used as often as more popular projective instruments such as the Rorschach and TAT. (2) SCTs are generally believed to assess a subject’s wishes, desires, fears, and attitudes about him- or herself and about significant relationships. As we have seen with many projective procedures, emphasis on content interpretation tends to overshadow evaluation of structural aspects of performance. (3) The development of a variety of different SCTs has all but precluded the acceptance of a single stimulus set of sentence stems. (4) Finally, and relatedly, there is no uniform scoring system for the SCT. Taken together, these reasons have probably both limited the utility and interest in SCTs as research instruments and clinical techniques.
One thorough review by Goldberg (1965) indicated that responses to sentence stems can be subjected to either a formal or content analysis. Formal variables include: (1) length of completion, (2) use of personal pronouns, (3) time for reaction and completion, (4) absolute and relative frequencies of parts of speech, (5) range of words used in relation to number of words used, and (6) grammatical errors, nonsensical responses, or neologisms. One study (Wilson, 1949) did not find that any of these factors differentiated groups of healthy and disturbed children.
Nonetheless, some of the conceptual principles reviewed thus far may serve as guidelines for thinking about how thought disorder is manifested on SCTs. The broad distinction between form and content is useful to identify some characteristics of response content that may signal disturbed thinking and reality testing. Completions that contain blatantly sexual, aggressive, or crude thematic content may reflect either characterological or psychotic impairment, depending upon the individual’s mindset and intentionality. As a general rule, we are interested in learning whether the individual includes bizarre or inappropriate content in his or her response in a willful or involuntary manner.
Putting content interpretation aside, can sentence completion response properties be conceptualized in a manner consistent with the framework laid down in this chapter as it has been applied to other projective techniques? As a point of departure, let us return to Rapaport’s concept of “close and distant reactions” (Rapaport et al., 1944–1946) as he applied it to the Word Association Test.
Rapaport included Jung’s Word Association Test (Jung, 1906–1915) among his standard battery of diagnostic tests. Although Word Association Tests are not a part of the mainstream of projective techniques, they share certain similarities in common with SCTs. Recall that Rapaport used the terms close and distant reactions to provide a psychological rationale for evaluating responses to the Word Association Test. By close and distant reactions, he was referring to interferences in the associative process from the stimulus word to the reaction (i.e., the first word that the subject could think of). Rapaport pointed out that in response to the test instructions, the healthy ego allows for conceptually related ideas to the stimulus to come to consciousness. The character of the usual associations is dictated by the test instructions “say the first word that comes to your mind” and results in a conventionally and conceptually related reaction word. According to Rapaport, unusual word associations can be classified as either “close” or “distant” reactions, depending on whether the individual sticks to the stimulus word “too closely” or in a loose and unrelated manner. Once again, the closenessdistance dimension calls to mind Schuldberg and Boster’s (1985) dimensions contrasting stimulus-bound and rigid response sets, on the one hand, with fluid and overly personal sets, on the other. As examples of overly close reactions to the stimulus word, Rapaport included reactions such as (1) repetition of the stimulus word, (2) perseveration of a previous response word, (3) clang responses, (4) selfreference, (5) multiword responses, and (6) senseless extensions of the stimulus word. Distant reactions included idiosyncratic and unrelated words.
Although the formal properties of SCTs differ from those of the Word Association Test, Rapaport’s concept of close and distant reactions may have some applicability to thinking about thought disorder on SCTs. What follows is a suggested typology of deviant types of responses, or completions, on the SCT that follows Rapaport’s ideas and is consistent with the generic typology proposed earlier in the chapter.
1. Close sentence completions. The subject responds to the sentence stem by simply repeating or partially repeating the stem. For example, to the stimulus sentence stem “My father . . .” the subject responds, “is my father.” The subject may also perseverate and respond with the same response completion to several of the sentence stems. As with the
Word Association Test, the subject may even respond to the sentence stem with a clang response, based on the sound of one of the words in the stem. All of these would be examples of Rapaport’s close reactions.
2. Distant sentence completions. These are idiosyncratic responses that are not clearly related to the sentence stem. An example of a completion response that is distant from the sentence stem would be (Stem): “When she saw that the boss was coming, Jane . . .” (Completion): “always bought carrots for dinner.” With inquiry, one may be able to make some sense out of the subject’s response; however, the fact that inquiry is needed indicates some failure in communicating meaning.
3. Deviant verbal expression (Peculiar Completions, Disorganized Completions, Incoherent Completions, and Impoverished Completions). As with any technique where words are used to convey meaning, disordered thought may be manifest by unusual word usage, disorganized syntax, incoherence, or impoverished verbal expression. SCTs, like all of the projective procedures discussed thus far, provide a means for assessing the nature of an individual’s formal thought organization as expressed through verbal expression.
4. Condensed completions. Though rare, condensed or contaminated thinking reflects a combination of primarily perceptual, verbal, and conceptual processes (Kleiger, 1999). Perceptually, images or details can be merged together, as in Rorschach contamination responses. Verbally, words can be condensed creating neologistic amalgamations. Conceptually, distinct categorical frames of reference can be collapsed in a manner that is unrealistic and bizarre, without accompanying perceptual or verbal condensation. Either verbal or conceptual condensations could signal severe thought disorder on the SCT. The appearance of a single neologism in an SCT completion response would be a red flag for the suspected presence of a thought disorder. Purely conceptual contaminations may also appear in SCT completion responses. Here there may be no dramatic neologistic condensation that immediately strikes the listener as bizarre. Instead, there is a merger between two incompatible frames of reference that logically contradict each other. For example, one might imagine a hypothetical response to the sentence stem, (Stem): “A wild animal . . .” (Completion): “becomes wild when it is tame.” Although somewhat poetic sounding, the completion collapses incompatible concepts in an illogical manner.
5. Vague and confused completions. Vague completions, like impoverished ones, may reflect the subject’s defensiveness, disinterest, or incapacity to formulate a meaningful response. Written or verbal expression of confusion with either the sentence stem or one’s completion may be similar to the perplexity that characterizes some organic conditions. Subjects who cannot understand the task or make sense out of the incomplete sentences are revealing their cognitive deficits in their inability to manage the inherent demands of the task.
6. Overly symbolic completions. Confabulatory thinking can fuse the completions to the stems in a manner that is inappropriately abstract and symbolic. Responses such as (Stem): “When he found out that he was not invited to the party, John . . .” (Completion): “knew that it was a sign of disconnection and alienation in society” reveal an internal preoccupation with a theme that becomes inappropriately attached to a stimulus.
CONCLUSIONS
Projective techniques offer a rich source of information about the structure and dynamics of mental functioning. With the exception of the Rorschach, these techniques are too often used only for assessing personality dynamics or mental representations through an examination of response content. Formal features of the responses—how the story was told, how the inkblot is seen, or how the figure is drawn—provide important information about thought organization and reality testing.
Departing from a sign approach to identifying thought disorder, one can conceptualize disordered thinking as a set of overlapping types of deviant cognitive processes that can manifest themselves similarly on different projective tests. The generic typology presented here borrows from other conceptual and categorical approaches to serve as a framework for thinking about how disordered thought is manifested on projective tests.
There are a number of promising avenues for empirical studies to pursue in the study of thought disorder assessment. Developing formal scoring systems for capturing manifestations of disordered thinking is a place to begin. From there, investigations into the diagnostic utility of these instruments and scoring approaches could follow. Redirecting a portion of research interest from the well-studied Rorschach to some of the other more neglected projective instruments could contribute to the diagnostic utility of these instruments and deepen our understanding of disordered thinking as well.
REFERENCES
- Andreasen, N.C. (1978). The Scale for the Assessment of Thought, Language, and Communication (TLC). Iowa City: University of Iowa Press.
- Arieti, S. (1974). Interpretation of schizophrenia. New York: Brunner.
- Buck, J.N. (1966). The House-Tree-Person Technique: Revised manual. Beverly Hills, CA: Western Psychological Services.
- Coleman, M.J., Carpenter, J.T., Waternaux, C., Levy, D.L., Shenton, M.E., Perry, J., et al. (1993). The Thought Disorder Index: A reliability study. Psychological Assessment, 5, 336–342.
- DiLeo, J.H. (1973). Children’s drawings as diagnostic aids. New York: Brunner/Mazel.
- Exner, J.E. (1993). The Rorschach: Volume 1 (3rd ed.). New York: Wiley.
- Exner, J.E. (2000). A primer for Rorschach interpretation. Asheville, NC: Rorschach Workshops.
- Exner, J.E., Weiner, I.B., & Schuyler, S. (1976). A Rorschach workbook for the Comprehensive System (4th ed.). Asheville, NC: Rorschach Workshops.
- Fish, F.J. (1962). Schizophrenia. Bristol, England: John Wright & Sons.
- Goldberg, P.A. (1965). A review of sentence completion methods in personality assessment. In B.I. Murstein (Ed.), Handbook of projective techniques (pp. 777–821). New York: Basic Books.
- Goldstein, K., & Scheerer, M. (1941). Abstract and concrete behavior: An experimental study of special tests. Psychological Monographs, 53, 1–151.
- Handler, L. (1985). The clinical use of the Draw-A-Person Test (DAP). In C.S. Newmark (Ed.), Major psychological assessment instruments (pp. 165–216). Boston: Allyn & Bacon.
- Harrow, M. & Quinlin, D. (1985). Disordered thinking and schizophrenic psychopathology. New York: Garden Press.
- Holt, R.R. (1956). Gauging primary and secondary process in Rorschach responses. Journal of Projective Techniques, 20, 14–25.
- Holt, R.R. (1977). A method for assessing primary process manifestations and their control in Rorschach responses. In M.A. Rickers-Ovsiankina (Ed.), Rorschach psychology (2nd ed., pp. 375–420). New York: Krieger.
- Holt, R.R., & Havel, J. (1960). A method for assessing primary and secondary process in the Rorschach. In M.A. Rickers-Ovsiankina (Ed.), Rorschach psychology (pp. 263–318). New York: Wiley.
- Johnston, M.H. & Holzman, P. (1979). Assessing schizophrenic thinking. San Francisco: Jossey-Bass.
- Jung, C.G. (1906–1915). Studies in word association. New York: Moffat Yard, 1919.
- Kissen, M. (1981). Inferring object relations from human figure drawings. Bulletin of the Menninger Clinic, 45, 43–54.
- Kleiger, J.H. (1999). Disordered thinking and the Rorschach. Hillsdale, NJ: Analytic Press.
- Lezak, M. (1976). Neuropsychological assessment. New York: Oxford University Press.
- Lindzey, G. (1961). Projective techniques and cross-cultural research. New York: Appleton-Century-Crofts.
- Machover, K. (1949). Personality projection in the drawings of the human figure. Springfield, IL: Charles C. Thomas.
- McElhaney, M. (1969). Clinical psychological assessment of the Human Figure Drawing. Springfield, IL: Charles C. Thomas.
- Piotrowski, Z.A. (1937). The Rorschach ink-blot method in organic disturbances of the central nervous system. Journal of Nervous and Mental Disease, 86, 525–537.
- Rapaport, D., Gill, M.M., & Schafer, R. (1944–1946). Diagnostic psychological testing (Vol. 2). Chicago: Year Book.
- Schuldberg, D., & Boster, J.S. (1985). Back to Topeka: Two types of distance in Rapaport’s original Rorschach thought disorder categories. Journal of Abnormal Psychology, 94, 205–215.
- Shenton, M.E., Solovay, M.R., & Holzman, P. (1987). Comparative studies of thought disorders II: Schizoaffective disorder. Archives of General Psychiatry, 44, 21–30.
- Solovay, M.R., Shenton, M.E., & Holzman, P. (1987). Comparative studies of thought disorders I: Mania and schizophrenia. Archives of General Psychiatry, 44, 13–20.
- von Domarus, E. (1944). The specific laws of logic in schizophrenia. In J.S. Kasinin (Ed.), Language and thought in schizophrenia (pp. 104–114). New York: Norton.
- Weiner, I.B. (1966). Psychodiagnosis in schizophrenia. New York: Wiley.
- Wilson, I. (1949). The use of a sentence completion test in differentiating between well-adjusted and maladjusted secondary school pupils. Journal of Consulting Psychology, 13, 400–402.
Back to top
Comment
Early research suggests conflicting evidence of the utility of the measurement of the MOAS for object relations in adults, as noted by Stricker and Healey (1990). However, more recent research supports the use of the MOAS as a valid assessment of object relations in adults.